![]()
![]()
![]()
In post-emergency situations the term “rehabilitation” is freely applied to a multiplicity of interventions and strategies. The distinction between an intervention which rehabilitates and an intervention which takes place during a rehabilitation or recovery phase is frequently blurred. This contributes to the tendency to regard rehabilitation as a half-way point along an emergency - rehabilitation - development sequence and often detracts from seeking more durable solutions to emergency situations.
“You can't do development in an emergency” is a familiar cry which, nevertheless, stands in sharp contrast to the UN Resolution 46/182, acknowledging a “clear relationship between emergency, rehabilitation and development”.5 This resolution, furthermore, emphasizes the need to ensure a smooth transition from relief to rehabilitation and development by providing emergency assistance which is supportive of recovery and long-term development. Thus, emergency measures should be seen as a step towards long-term development. Despite being a worthwhile objective, the linking between relief and development is often difficult to achieve, in particular in conflict situations.6
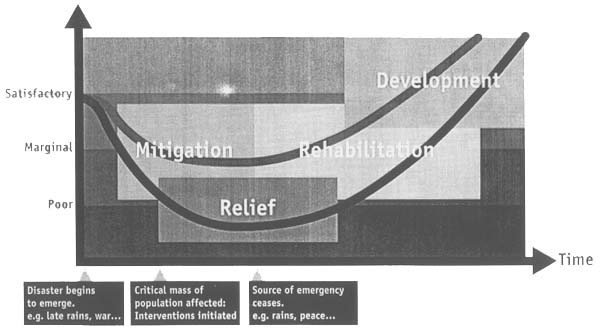
The concept of rehabilitation and the model of the relief-to-development continuum (figure 1) in this paper rests on a clear division between the type and timing of a response. The continuum relates to the effects of the intervention on the affected households or populations.
Figure 1: The relief-to-development continuum
Nutrition Security
Household Food Security
Adapted from WILLIAMS, C. Agriculture, food and nutrition in post-emergency and rehabilitation - Issues, needs and interventions. February 1994 (draft)
The International Conference on Nutrition (ICN) defined food security as “access by all people at all times to the food needed for a healthy life”. At the household level this rests on the sustainable ability of the household to secure adequate food of appropriate nutritional composition from its own production or purchases.7
Since household food security is primarily concerned with access to nutritionally adequate food at household level, its achievement may not necessarily result in improvements in the nutritional status of all household members. This is due to several assumptions which cannot be met by most of the present food security interventions:
having access to food does not assure adequate consumption by all households in need,
adequate overall consumption by households does not assure adequate consumption by vulnerable individuals within households,
adequate energy consumption by households and vulnerable individuals does not guarantee diet quality and safety sufficient to produce nutritional well-being, and
the consumption of adequate food does not void the important role of non-food factors in the biological utilization of food.8
Nutrition security, instead, focuses on the nutritional wellbeing of the individual household member; the concept of nutrition security is concerned with the consumption and physiological utilization of adequate quantities of safe and nutritious food by each individual member of the household.
Figure 2 summarises both, the factors influencing household food security and the various determinants of nutrition security. It also illustrates the interactive relationship between the two conditions and underlines the pivotal role which nutrition security plays in the endeavours of people to make a living.
It becomes apparent that nutrition security is influenced by a complex set of processes operating at the level of the household unit, within it, and at the level of its individual members. Household food security is one prerequisite for nutrition security.9
Figure 2: Determinants of household food security and nutrition security
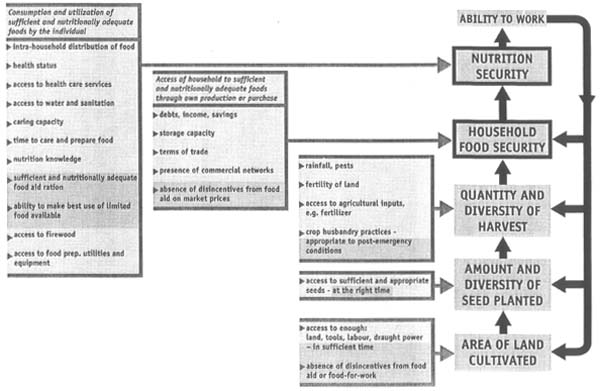
Note: Factors which only apply during rehabilitation are shaded
Adapted from WILLIAMS, C. Agriculture, food and nutrition in post-emergency and rehabilitation - Issues, needs and interventions. February 1994 (draft)
An appreciation of the determinants of and differences between household food security and nutrition security explains why improving household food security is not a guarantee for reducing malnutrition. Wealthier, food secure households can still have malnourished children, and low-income, (partly) food-insecure households can have well-nourished children if they prioritise child feeding10.
From the discussion above, it is apparent that developing rehabilitation programmes to improve nutrition status requires addressing the specific constraints to nutrition security and recognition that these may be different from the constraints to household food security. This is illustrated further in section 4.
![]()
![]()
![]()