


Contagious bovine pleuropneumonia (CBPP lung sickness) caused by Mycoplasma mycoides subspecies mycoides is one of the most economically important diseases occurring in Namibia.
The disease is considered endemic in the northern central and Kavango regions and sporadic in the Kunene region. The commercial farming areas south of the veterinary cordon fence (VCF) and the Caprivi region are free from infection. CBPP has remained a notifiable disease in Namibia since 1887. Vaccination and movement restrictions are the main methods employed to limit the effects of the disease and its spread to free areas. The report is aimed at highlighting the disease trend since vaccination with T144 vaccine was begun in mid-1997. The analysis is based on data received through the official veterinary reporting system.
On the advice of international experts, countrywide vaccination of cattle with T144 vaccine was implemented. The strategy was to have two vaccinations within the first years followed by single annual campaigns for a period of at least five years during which 100 percent of all cattle at risk would be vaccinated. The aim of this strategy is to reduce the disease prevalence to such a level that continued transmission of the infection becomes unlikely. In the absence of a continued influx of unvaccinated animals from across the border, vaccination could then be stopped and intensive surveillance implemented for remaining pockets of infection which would be sought and eliminated. This phase of CBPP control was restarted with a vaccination campaign in June 1997, followed by a second campaign in 1998 and a third in 1999.
The high-risk areas are considered to be Ondangwa (northern central), Rundu and Opuwo. The movement of animals from southern Angola is believed to play an important part in maintaining infection in these areas. Where such movements are detected, the animals are vaccinated. No CBPP has been diagnosed in eastern Caprivi since it was eradicated in 1938 but cattle in the Katima Mulilo state veterinary district are vaccinated to protect them from possible infection with CBPP from Western Province, Zambia.
The table below shows the number of cattle vaccinated and as a percentage of the population at risk covered during the campaigns in different regions since 1997.
Region |
1997 |
1998 |
1999 |
Katima (Caprivi) |
13 986 (87%) |
15 126 (94%) |
20 343 (96%) |
Rundu |
99 679 (87%) |
93 051 (82%) |
107 731 (95%) |
Ondangwa |
389 472 (82%) |
543 550 (114%) |
626 062 (115%) |
Opuwo |
136 387 (80%) |
165 216 (98%) |
133 953 (75%) |
Overall, the vaccination coverage since 1997 has been very good. In some cases, more cattle than the resident population were vaccinated. It is believed that some Angolan animals are moved across the border into Namibia to take advantage of the preventive vaccination. This suggests that stock owners in that country have confidence in the protection offered by vaccination.
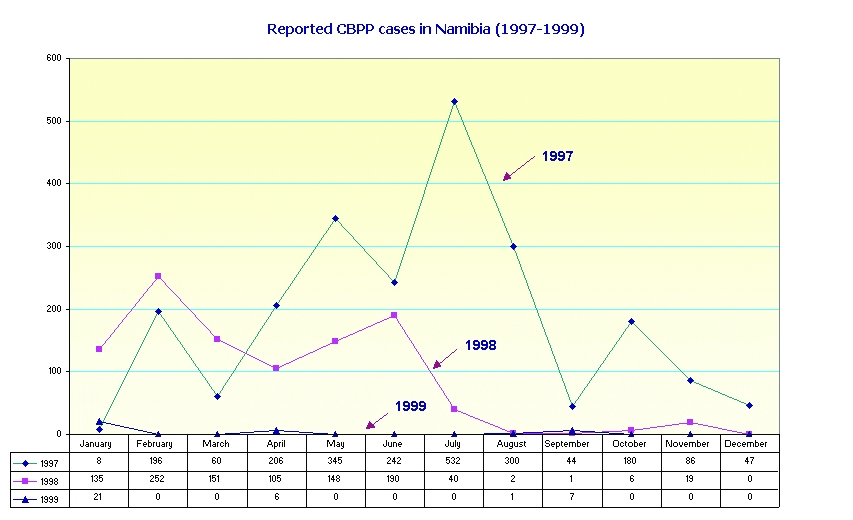
a) Monthly incidence
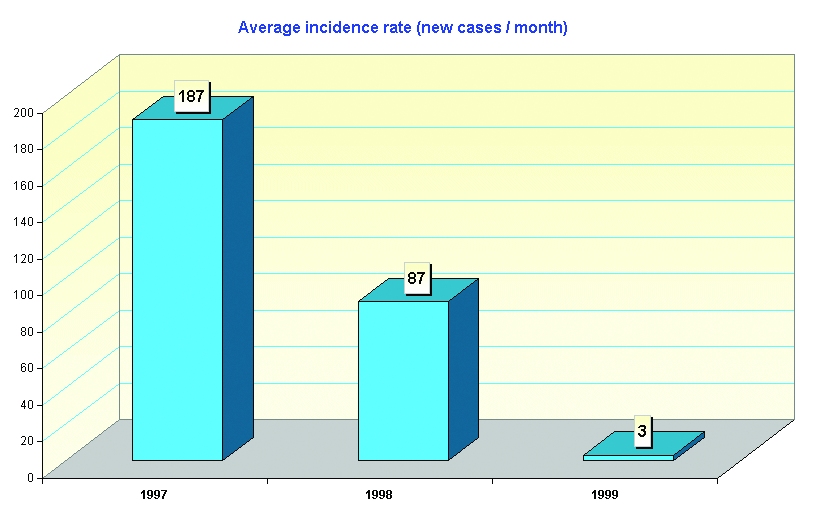
The data suggest a progressive and significant reduction in disease incidence since 1997. The monthly CBPP incidents (cases) reported since the current campaign started are shown in Figure 1. It can be noted that the cases reported have dropped from an average of 269 to 16 per month (Figure 2). There has been a corresponding decrease in outbreaks and deaths (Figure 3). If vaccination is continued for a few more years and the downward trend continues, the stage will be set for the eradication phase. Unfortunately, this is unlikely to be achieved in the foreseeable future unless movements from Angola can be controlled. This leaves only the option of implementing the same strategy in Angola and other affected countries with the aim of eradicating the disease on a regional basis.
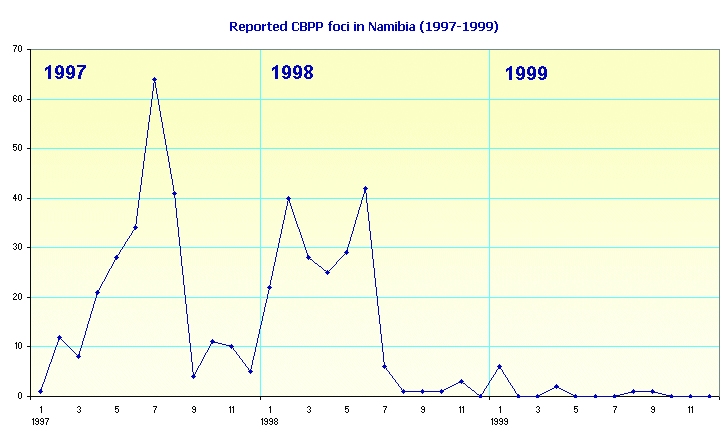
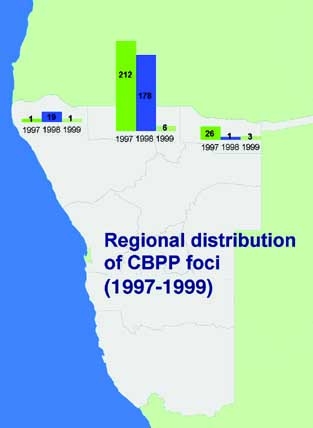
b) Morbidity and geographical distribution
The number of CBPP foci reported from the different regions are shown in the map below.
Although the current disease trend is very encouraging, it must be viewed with caution because the disease data are based on passive surveillance. Active surveillance is required to make a better assessment of the disease status. This requires accurate identification of individual herds, sources of infection, traceability of origins of infections and all contact herds. Cases detected at the abattoir must also be traceable. The recent introduction of individual brands in infected areas will help in this regard.
Valuable data can be obtained from examining lungs at slaughter. In the case of high-risk regions, animals go through quarantine before slaughter, thus eliminating visibly infected animals. Farmers also tend to withhold these animals for fear of losses following outright condemnation. For local use, most animals are slaughtered at "bush" abattoirs where there is no veterinary supervision. Potentially useful and additional CBPP prevalence data from these informal slaughter places are thus missed.
The lack of fences and the pastoral semi-nomadic farming system in the northern communal areas make control of movement (an essential element in eventual eradication) difficult. It is imperative that stock owners are informed of the downward trend of CBPP, that they continue bringing all their animals for vaccination and that they are encouraged to report all clinical and post-mortem cases so that all the data are captured. Treatment of animals with antibiotics masks CBPP and must be discouraged. Cross-border animal movements will remain the major obstacle to achieving the goal of eradication and must be discouraged until the health status of animals in southern Angola is at par with that in Namibia through regionally coordinated efforts.
(Contributed by: Dr Cleopas Bamhare and Ms Bertchen Kohrs, Epidemiology Unit, Directorate of Veterinary Services, Windhoek, Namibia.)