![]()
![]()
![]()
A hypothetical pattern of an epidemic over time can be represented with a highly stylized s-shaped or logistic curve (figure 1). In the initial stages of the epidemic, the HIV prevalence is quite low and is followed by a period of acceleration (stage I to stage II) where the virus is spreading at a rapid rate throughout the population. This stage of acceleration is followed by a period of slowing growth where the numbers of new infections stabilize, but a high proportion of the population at risk already has been infected (stage III). Eventually both new infections and the proportion of infected should decrease.
The HIV epidemic is particularly devastating as people do not leave the HIV infected population by getting better, but by dying. Consequently, the epidemic curve that represents HIV infection can be followed by a similar curve a number of years later which represents the accumulation of those who died from AIDS-related causes.
The pattern of the epidemic varies between regions and within countries; the epidemic may level off in some countries at modest levels, while in others, sizeable proportions may be infected before an upper limit is reached. In southern Africa, for example, HIV rates are still rising, with HIV infection among more than 40 percent of all pregnant women in some locations. In West Africa, the apparent stability of the epidemic has turned out to be a misconception, with the prevalence rates now taking off again (UNAIDS 2002). In spite of variations in epidemic patterns, it is important for the agricultural sector to recognize that countries and regions can be at different stages of the epidemic and may need different response strategies.
Figure 1. Stages of the epidemic
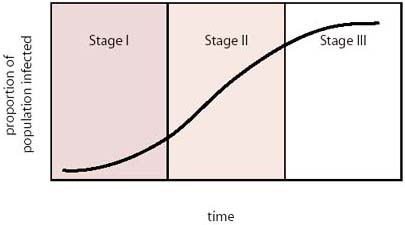
Source: Barnett, T. (2001)
It is estimated that 42 million people in the world are infected with the HIV virus and 95 percent live in developing countries (UNAIDS 2002). Assuming that each HIV/AIDS case directly influences the lives of four other individuals, at least 160 million people are likely to be affected by the epidemic (Barnett, Whiteside 2002). With more than two-thirds of the population of the 25 most affected African countries living in rural areas and largely dependent upon agriculture as a means of subsistence, any HIV/AIDS mitigation strategy has to encompass the livelihoods of rural agricultural populations (FAO 2002a).
Rural farming systems are comprised of a diverse range of tasks which generate both farm and off-farm income. Households are becoming increasingly dependent upon off-farm sources, in particular cash income or remittances from migrant labour, whether to buy farm inputs or pay school fees. These structural forces forge dynamic links between rural and urban areas, increasing their interdependence and serving as a channel for the flow of cash, people and as a route for all infectious disease, including the transmission of HIV.
| HIV/AIDS and mobility |
| Mobile people are those who move from
one place to another temporarily, seasonally or permanently for a host of
voluntary or involuntary reasons. They include truck drivers, seafarers,
transport workers, agricultural workers, business people, traders, employees
of large industries, miners, government officials, uniformed service officers,
construction workers and sex workers.
Internal migrants move within their country of birth and include rural-urban movements and resettlement, whereas external migrants cross country borders. While being mobile itself is not a risk factor for HIV, the situations encountered and the behaviours adopted during the mobility process may increase a person’s vulnerability to the disease, for example:
People are also affected by mobility through interaction with others who are mobile even if they are not mobile themselves and so become vulnerable to the risk of HIV transmission. They include spouses, children and the elderly. Source: UNDP (2001) |
Poverty and mobility are critical dimensions of vulnerability to HIV transmission. The driving force behind migratory movements is poverty, in addition to the lack of livelihood opportunities in rural areas. Migrant workers who are away from home for extended periods of time are more likely to engage in casual, unprotected sex, thus increasing their risk of exposure to HIV transmission.
The agricultural sector plays an important role in influencing migratory patterns. Many commercial estates employ large numbers of seasonal migrant workers. The accommodation that is provided on commercial estates tends not to support the families of workers, are often over-crowded, lack privacy and provide situations that are conducive to casual and commercial sex. In addition, small farmers who are involved in cash crop production often have to travel to complete marketing arrangements and buy new inputs. Infrastructure projects facilitate agricultural production and marketing but also encourage high levels of labour mobility and temporary migration.
Those less mobile groups who remain in rural areas have to manage the impacts of the HIV epidemic with a dwindling resource base. Those without land, or with marginalized land and fragile farming systems are far less able to cope with the impacts of HIV/AIDS, and as an increasing number of sick HIV-infected urban dwellers return to their rural communities, survival strategies become stretched and food security threatened. Rural populations are at a further disadvantage as they have little access to appropriate information and health services and so are less able to equip themselves with the knowledge to prevent the risks of transmission.
The major impacts of HIV/AIDS on food security and rural livelihoods are summarized in table 2 and some of the most important are outlined in the following paragraphs.
Demographic projections of the impact of HIV/AIDS on population structures reveal dramatic changes in the size, age and sex compositions (figure 2). Not only will the total population be reduced, but the projected age and sex structure will change, resulting in a population dominated by the elderly and the youth. In many countries, AIDS is erasing decades of progress made in improving mortality conditions and extending life expectancies. The average life expectancy in sub-Saharan Africa is now 47 years, when it would have been 62 years without AIDS. In Botswana, for example, life expectancy at birth has dropped to a level not seen in this country since 1950 (UNAIDS 2002).
Figure 2. Projected population structure with and without the AIDS epidemic, Botswana 2020
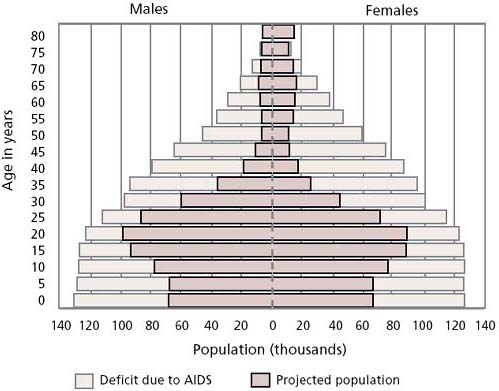
Source: United States Census Bureau, World Population Profile (2000)
HIV/AIDS poses a direct threat to household food security as it affects the most productive household members. When a person is sick the household not only has to manage without their labour inputs but with the loss of labour from those who have to care for the sick. AIDS is characterized by recurrent periods of sickness, and so recurrent loss of labour, which eventually erodes agricultural production and food security. Much of rural agricultural production is highly labour-dependent and often labour demands are concentrated in specific periods of the year. For instance, sickness or funeral attendance may mean that the planting season is missed and with it, a full crop.
Gross agricultural production is also affected by labour shortages. The FAO has estimated that in the 25 hardest hit countries in Africa, AIDS has killed around 7 million agricultural workers since 1985 and it could kill 16 million more before 2020. The most affected African countries could lose up to 26 percent of their agricultural labour force within a few decades and with agriculture still representing a large proportion of the gross domestic product, this loss in labour could have severe impacts on the national economy (FAO 2001b).
| Table 1. Projected loss in total population and agricultural labour force due to AIDS, 1985-2020 | ||
| |
Total population |
Agricultural labour force |
|
Namibia |
-17% |
-26% |
|
Botswana |
-30% |
-23% |
|
Zimbabwe |
-23% |
-23% |
|
Mozambique |
-16% |
-20% |
|
South Africa |
-27% |
-20% |
|
Kenya |
-16% |
-17% |
|
Malawi |
-17% |
-14% |
|
Uganda |
-8% |
-14% |
|
Tanzania |
-7% |
-13% |
Source: FAO (2001b)
Rural farming systems depend upon a wealth of local agricultural and biodiversity knowledge that is essential for maintaining production. The loss of a productive generation means that livelihood skills including agricultural knowledge are not passed from generation to generation, leaving a young population ill-equipped to manage the impacts of the epidemic. Moreover, agricultural skills are often gender-specific and the sickness or death of a male or female household member can result in a weakening of the farming system.
| HIV/AIDS and the impact on smallholder agriculture in Zimbabwe |
A study of the impact of HIV/AIDS on
smallholder agricultural production in Gweru, Zimbabwe found that:
Source: Ncube, NM. (1999) |
HIV/AIDS has direct impacts on nutrition for the individual, the household and the community. For the individual, HIV infection, compounded by inadequate dietary intake, rapidly leads to malnutrition. Persons living with HIV have higher than normal nutritional requirements; approximately 50 percent more protein and 10-15 percent more energy per day is needed (Academy for Educational Development 2001, Woods 1999, James, Schofield 1990). Such interactions have serious consequences for the poor, who are more likely to be malnourished even before they become infected. Malnutrition may hasten the onset of AIDS and ultimately death, and may also increase the risk of vertical HIV transmission from mother to child. The re-occurring periods of sickness of those living with HIV place a strain on the availability of farm labour and, if sustained, on household food production and ultimately the nutritional status of other household members.
The rural and agricultural dimensions of the HIV/AIDS epidemic not only present devastating impacts on agricultural production, but also reduce the capacity of rural institutions to provide adequate services. The first impact experienced by formal organizations is a decline in human resources, as more staff are absent due to repeated periods of AIDS-related sickness. The quality of the service is affected as other staff members have to cover for their colleagues’ absence, thus increasing their own workload and decreasing the geographical area which mobile staff, such as extension workers, are able to cover. Organizations also suffer from less tangible results of increasing staff attrition. Certain technical skills can be replaced, but institutional knowledge and experience cannot be easily substituted with new staff. In addition, there are direct budgetary costs associated with continual attrition that can divert organizations’ funds away from operational activities. Informal institutions are also affected by a dwindling contribution from AIDS afflicted households. Constraints on these households’ time and resources reduce their ability to participate in these community networks and in turn, reduce their access to these vital social safety nets and so increase their vulnerability.
Gender inequality is one of the driving forces behind the spread of HIV. In order to adequately address gender, it is necessary to consider the wider social, economic, political and cultural context in which inequalities are generated and maintained.
In many places HIV infection rates are three to five times higher among young women than young men. These differentials in HIV infection are partly explainable by biological factors which make women more vulnerable to HIV, especially in youth and adolescence. HIV differentials also reflect age differences between sexual partners, in which men are older and more dominant and tradition and social pressures limit women’s ability to express their wishes regarding their sexuality, their choice of sexual partners and their ability to demand protected intercourse, thus increasing their risk of contracting HIV.
Gender inequalities render women more vulnerable to the effects of the HIV/AIDS epidemic. Rural women’s domestic work loads tend to increase, as they are often the care providers when household members are sick. Access to productive resources, including land, credit, training and technology are strongly determined by gender and frequently favour men in the allocation of resources. As the household asset base dwindles and more members become sick, women’s access to scarce resources is further diminished. Moreover, following the death of a spouse, a widow may not be granted access to household resources resulting in further impoverishment.
| Female farmers and HIV/AIDS |
Source: FAO (2002a) |
HIV/AIDS, agriculture, food security, rural poverty and mobility, form a complex matrix of inter-relationships and competing forces. The success of any HIV mitigation strategy would depend upon its ability to recognize this wider environment in designing interventions. The livelihoods framework (figure 3) is a useful analytical tool for organising these competing influences and understanding the impact on rural livelihoods. The framework also aims to help different stakeholders engage in a structured and coherent debate. It presents the main factors that affect people’s livelihoods, their relative importance and the way in which they interact to form survival strategies.
Households are seen to possess five sets of livelihood assets essential to their livelihood strategies: human capital, natural capital, financial capital, social capital and physical capital. Utilizing these assets, households adjust to their physical, social, economic and political environments through a set of livelihood strategies designed to strengthen their well being. The contexts in which households operate involve threats that render them vulnerable to negative livelihood outcomes. These threats can include periodic droughts, floods, pest infestations, crop and livestock shocks, economic shocks, conflict and civil unrest, as well as the illness and death of household members.
Figure 3: The livelihoods framework
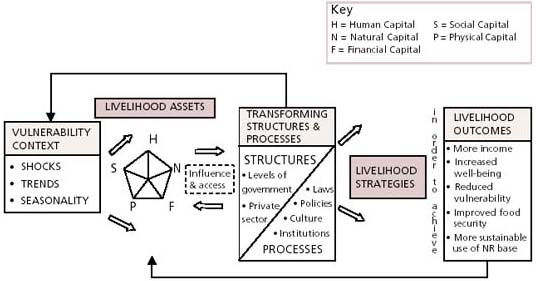
Source: DFID, FAO (2000)

FAO/J. Holmes
In reference to the diagram shown in figure 3, HIV/AIDS represents a potentially devastating shock to the farm household. The illness or death of one or more household members can affect each of the livelihood assets resulting in a reduction in the ability of the household to adjust to future shocks. This situation, combined with unfavourable structures and processes (represented to the right of the asset pentagon), could result in livelihood strategies that are not sustainable and outcomes that impact a household’s ability to respond and maintain long-term food security.
| AIDS orphans, the situation is critical |
Source: FAO (2001b) and UNAIDS, USAID, UNICEF (2002) |
Table 2: The impact of HIV/AIDS on food security and the implications for households and communities
|
Impacts of HIV/AIDS on food security |
Implications |
|
Dramatic changes in the population |
Increase in orphaned children Proportional increase in the elderly Increase in widows and female-headed households |
|
Decrease in the agricultural labour force |
Decrease in the area cultivated, in weeding, pruning and mulching, resulting in a decline in crop variety, yields and ultimately soil fertility Increase in fallow land returning to bush Less labour intensive cropping patterns and animal production Decrease in women’s productive activities due to their role as care providers Missed planting seasons |
|
Chronic illness or death of a household member |
Increase in health expenditure Funeral costs |
|
Change in household composition |
Changes in the age or sex of the household head Increase in the household dependency ratio Out-migration of young adults |
|
Increase in the number of orphaned children |
Increase in the fostering of orphaned children Child headed households resulting in reduced attendance or withdrawal of children from school |
|
Change in household nutritional status |
Increase in the malnutrition of people living with AIDS and other household members due to the increasing impoverishment of the household |
|
Acute decline in household income |
Decrease in farm income sources and the proportion of farm output marketed Sale of land Liquidation of savings and slaughtering of livestock to provide income for health care and funerals Decrease in women’s contributions to household income Decline in purchased items including food Increased need for cash income sometimes resulting in sex work Increase in the need for off-farm income sources |
|
Decrease in credit availability and use |
Increase in interest rates and more frequent loan defaults |
|
Decrease in aggregate community income and assets |
Reduction in investment |
|
Loss of agricultural knowledge, practices and skills and their transmission from one generation to the next |
Decrease in the availability of skilled labour and essential agricultural knowledge for orphan-headed households Loss of gender-specific agricultural knowledge |
|
Decrease in access to natural resources, especially land |
Depletion of resources in close proximity to households, especially water and forest assets Decrease in biodiversity and the pool of genetic resources |
|
Exacerbation of gender-based differences in access to resources |
Increase in gender inequality, resulting in a decrease in access to land, credit and knowledge, for women in general, but particularly for widows |
|
Changes in social resources |
Less time available to participate in community-based organizations, associations and other support networks |
|
Increase in social exclusion |
Increased stigma associated with HIV, thus increasing the difficulty of maintaining social and kin groups |
|
Decrease in tangible household assets |
Poor household maintenance Increase in sale of household goods, equipment and tools |
|
Degradation of public services |
Reduction in the quality and quantity of public service provision Less maintenance of communal irrigation systems, terraces, roads |

FAO/A. Wolstad
![]()
![]()
![]()