![]()
![]()
![]()
Table 17 provides numbers of reported cases of the most serious communicable diseases. It is clear from the available data that hepatitis has been the most widespread and serious communicable disease in Egypt over the last 25 years, followed by pulmonary tuberculosis and meningococcal meningitis. There is also high mortality among patients with tuberculosis (TB), meningitis and hepatitis, but the compulsory vaccination programme against hepatitis B and the new prophylactic and therapeutic measures to control the spread of hepatitis C might have diminished the mortality among hepatitis patients (WHO, 2005).
In contrast, the relatively high mortality rate among AIDS patients, which does not correspond to the total of reported cases, may be due to difficulties in identifying cases before they reach their terminal phases when patients are quarantined in fever hospitals. In addition, a high mortality rate for a specific year may include AIDS patients who were infected and diagnosed over many of the previous years.
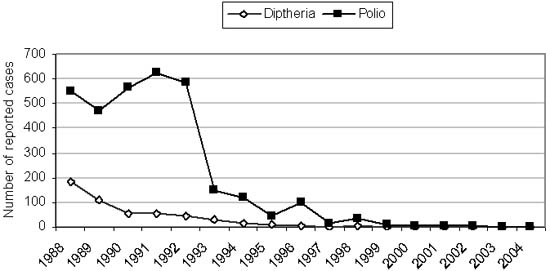
It is worth mentioning that the success of the Egyptian vaccination programme against diphtheria and poliomyelitis was the main cause of decreases in reported cases over recent years; the programme aims to eradicate these diseases completely (Figure 35).
Malaria is the most widespread and serious communicable disease in the world, and Egypt is among a group of countries with some remaining areas of transmission. The specific target for this disease is to eliminate the few remaining foci of malaria by 2006 (WHO, 2004).
TABLE 17
Numbers of reported cases of communicable
diseases in Egypt, 1980 to 2004
|
Year |
Malaria (P)1 |
Diphtheria |
Meningococcal meningitis |
Poliomyelitis |
Pulmonary tuberculosis |
HIV/AIDS |
Hepatitis |
|
1980 |
370 |
333 |
296 |
2 006 |
1 381 |
|
|
|
1981 |
|
|
|
|
|
|
|
|
1982 |
365 |
809 |
2 061 |
2 113 |
1 596 |
|
18 188 |
|
1983 |
|
|
|
|
|
|
|
|
1984 |
|
|
|
|
|
|
|
|
1985 |
72 |
663 |
848 |
564 |
1 143 |
|
17 185 |
|
1986 |
|
|
|
|
|
|
|
|
1987 |
|
|
|
|
|
|
|
|
1988 |
225 |
184 |
3 327 |
550 |
1 231 |
|
15 188 |
|
1989 |
192 |
110 |
3 894 |
474 |
1 394 |
|
14 009 |
|
1990 |
75 |
59 |
3 976 |
565 |
2 740 |
7 |
14 209 |
|
1991 |
24 |
55 |
1 210 |
625 |
1 531 |
12 |
|
|
1992 |
16 |
44 |
1 165 |
584 |
8 876 |
23 |
15 108 |
|
1993 |
17 |
29 |
896 |
150 |
3 416 |
29 |
|
|
1994 |
527 |
18 |
800 |
120 |
3 223 |
22 |
|
|
1995 |
313 |
10 |
671 |
47 |
9 708 |
16 |
|
|
1996 |
25 |
6 |
661 |
100 |
10 236 |
14 |
|
|
1997 |
11 |
1 |
167 |
14 |
11 040 |
25 |
|
|
1998 |
13 |
3 |
489 |
35 |
9 650 |
33 |
13 340 |
|
1999 |
61 |
2 |
419 |
9 |
8 878 |
34 |
|
|
2000 |
17 |
0 |
278 |
4 |
7 919 |
44 |
14 671 |
|
2001 |
11 |
0 |
201 |
5 |
7 900 |
33 |
|
|
2002 |
10 |
0 |
130 |
7 |
8 223 |
47 |
|
|
2003 |
45 |
0 |
|
1 |
|
|
|
|
2004 |
14 |
0 |
135 |
1 |
5 378 |
|
|
1 Malaria P = parasitological confirmed
malaria.
Source: WHO, 2005.
FIGURE 26
Numbers of reported cases of diphtheria and
poliomyelitis in Egypt, 1988 to 2004
|
|
The prevalence of antibody to hepatitis C virus (anti-HCV) was determined in a cross-sectional survey of a village in Upper Egypt (Medhat et al., 2000). Prevalence was higher among males than females, at 11.3 and 6.5 percent, respectively, p < 0.001. It was greater among those over 30 years of age than among those up to 30 years of age (20.0 percent versus 3.6 percent, p < 0.001). Hepatitis C virus RNA was detected in 62.8 percent of the anti-HCV-positive subjects, without significant variation by age, gender, education or marital status.
Abd El-Aziz et al. (2000) conducted a cross-sectional survey of the prevalence of anti-HCV in a rural community in the Nile Delta. Overall, 973 (24.3 percent) out of 3 999 residents were anti-HCV-positive, and the age- and gender-adjusted seroprevalence was 23.7 percent. Anti-HCV prevalence increased sharply with age, from 9.3 percent in those aged 20 years and under to more than 50 percent in those over 35 years. Of the 905 anti-HCV-positive samples tested, 65 percent were also positive for HCV-RNA. Active schistosomal infection was not associated with anti-HCV status, but a history of antischistosomal injection therapy was reported by 19 percent of anti-HCV positives.
The population of Egypt has a heavy burden of liver disease, mostly due to chronic infection with HCV. The overall prevalence of anti-HCV in the general population is about 15 to 20 percent. Egyptian parenteral antischistosomal therapy (PAT) mass-treatment campaigns discontinued only in the 1980s, and show a very high potential for transmission of blood-borne pathogens. A cohort-specific exposure index for PAT was calculated and compared with cohort-specific HCV prevalence rates in four regions. The data suggested that PAT had a major role in the spread of HCV throughout Egypt (Frank et al., 2000).
Infections among children
The morbidity load in Egypt, particularly in preschool children, is due mainly to diarrhoea and respiratory tract infections, as shown by statistics from MOHP, as well as many community-based research studies. Detailed studies of urban children under the age of three years revealed that diarrhoea was the cause of morbidity in 37.7 percent of cases in underprivileged areas in Cairo, and of 24.7 percent of cases in Alexandria; respiratory tract infections were responsible for 29.4 and 36.4 percent of cases in the two cities, respectively (Moussa et al., 1983).
Similar studies in rural areas (Galal, 1987) revealed that infants from birth to six months of age were ill for 25 percent of the time observed. Gastrointestinal and respiratory infections constituted, respectively, 37.9 and 31.8 percent of all infant illness. In the same study, toddlers aged 18 to 30 months fell ill an average of almost ten times a year, the total time span of illness averaging 11 percent of the year, but reaching as high as 30 percent. Approximately 40 percent of ailments were gastrointestinal in nature, and one-third respiratory infections.
The National Diarrhoeal Disease Control Programme reported that cases admitted to Bab El-Shaeiria hospitals with acute diarrhoea and dehydration were reduced by 71 percent in 1984 and by up to 75 percent in 1990. Existing data indicate that acute respiratory infection and diarrhoeal diseases were responsible for 30 and 16 percent, respectively, of infant deaths in 1999 (UNICEF, 2003).
Parasitic infestation
Moussa (1989) studied the relation between parasite infestation and malnutrition among schoolchildren aged six to 12 years in different nutritional grades, based on weight-for-age categories. The results revealed that urinary bilharziasis and ancylostoma were most prevalent among the group with third degree undernutrition; ascariasis was highest among the overweight group (but did not exceed 15 percent). Amoebiasis was least prevalent among the group of normal weight-for-age, and most prevalent among the overweight group.
The results of a survey to assess micronutrient deficiencies among primary schoolchildren in three governorates - Cairo, El-Sharquia and Quena - revealed that the highest prevalence of ascaris infestation was among rural boys in El-Sharquia governorate (14.3 percent). Oxyuris infestation was prevalent in the three governorates, with the highest prevalence in El-Sharquia (15.6 percent), followed by Cairo (11.1 percent) and Quena (6.9 percent). The highest prevalence of Schistosoma hematobium (urinary bilharziasis) was 10 percent among rural boys in Quena governorate (Hassan et al., 1998).
|
[6] This section was
investigated by A. El-Hady Abbas, S. Khairy and M. Shehata. |
![]()
![]()
![]()