![]()
![]()
![]()
Chapter 7 - Food, nutrients and diets
The major nutrients and their functions
Micronutrients: vitamins and minerals
Food and nutrient requirements for different ages and groups
Factors affecting energy and nutrient requirements
Vulnerable periods in the life cycle and special energy and nutrient needs
This chapter gives information on different foods, their nutrient content and their physiological role in the body, in addition to nutrient requirements and the factors affecting them. It reviews the composition of African diets and the different factors that may affect meal preparation and eating patterns. The chapter may be helpful for those wanting more detailed nutrition information. Some people concerned with agriculture and food-related nutrition issues, for example agriculturists and agricultural extension workers, may not need all of this information. Similarly, the public will not need all of the information provided here in order to prepare wholesome meals and maintain good nutritional and health status. A practical approach to healthy eating is simply to advocate consumption of a mixture of foods, focusing on a staple with added energy and protein sources and relish foods providing essential micronutrients.
Foods, like crops, can be classified and grouped in various ways. Agriculturists divide crops into field crops, plantation crops, commercial crops, horticultural crops, forage crops and grasses. Such groups usually overlap, and particular plants may appear in more than one group.
In nutrition, a number of different ways of grouping foods have been tried. Food groups may be based on the major nutrient content (e.g. fatty foods, starchy foods, protein foods); the role of the foodstuffs in human nutrition (e.g. energy foods, protective foods, body-building foods); individual nutrients (e.g. carbohydrates, fats, vitamins, protein); or commercial value (e.g. cereals, roots and tubers, nuts and seeds, fruits, leafy vegetables).
All foods from plants and animals contain a mixture of nutrients. Refined white sugar, which consists of 100 percent carbohydrate (sucrose), is the exception. While it is possible to classify some foods according to major nutrients, most foods fall into several categories (see Table 38).
The need for diversity in both production and consumption has been discussed in Chapters 4 and 5, especially in relation to household food security. Individual food security, expressed as a balanced and adequate diet, also depends on diversity. The basis of the advice often given in nutrition education for family meal planning is: "Select at least one food from each of the food groups". However, other factors including cost and acceptability must also be considered (see Box 52).
Table 38 - Nutrients in different types of foods
Food |
Rich source of |
Moderate source of |
Cereals |
Starch, fibre |
Protein, B vitamins, many minerals |
Starchy roots and fruits |
Starch, fibre |
Some minerals, vitamin C if fresh, vitamin A it yellow or orange |
Beans and peas |
Protein, starch, some minerals, fibre |
B vitamins |
Oilseeds |
Fat, protein, fibre |
B vitamins, some minerals |
Fats and oils |
Fat |
Vitamin A if orange or red |
Dark- to medium-green leaves |
Vitamins A and C, folate |
Protein, minerals |
Orange vegetables |
Vitamins A and C |
Fibre |
Orange fruits |
Vitamins A and C |
Fibre |
Citrus fruits |
Vitamin C |
Fibre |
Milk |
Fat, protein, calcium, vitamins |
|
Eggs |
Protein, vitamins |
Fat, minerals (not iron) |
Meat |
Protein, lat. iron |
|
Fish |
Protein, iron |
|
Liver |
Protein, iron, vitamins |
Source: King and Burgess, 1993.
Box 52 - Why teaching about the three food groups is not recommended In the past, health and nutrition workers used the idea of the "three food groups" (energy foods, body-building foods and protective foods) when they taught mothers how to plan meals. Now teaching about food groups is not believed to be the best way to help families improve their meals and prevent undernutrition, for the following reasons. Many foods belong to more than one group Most foods are mixtures of nutrients. Cereals are in the energy food group, but they are an important source of protein and B vitamins as well as starch. Milk is usually in the bodybuilding group, although it contains as much fat as protein, and it contains calcium and several vitamins. Groundnuts are also rich in both energy and protein. People need to eat both starch and fat Starchy foods and fatty foods are both in the energy food group, so it is not clear that people need both. A meal of one food from each group may not be balanced The concept of the three food groups suggests that a balanced meal could be made from margarine (an energy food), cheese (a body-building food) and a banana (a protective food), or from sugar, an egg and a lemon. These would be strange meals, and they would lack several nutrients. Important problems are left out The concept of the three food groups only addresses the mixture of foods. It does not explain about the amounts of food that people need, or about bulky weaning foods, or about feeding children often. Most women do not use the idea of the three groups Many women know about the three food groups, but most admit that they do not regard them, because they often cannot afford to buy the foods and they do not plan meals in that way. |
Source: Adapted from King and Burgess, 1993. |
Eating is a natural and essential activity. When there are constraints in the food system and access to food is restricted on economic, social or cultural grounds, basic nutritional needs for energy and essential nutrients may not be satisfied.
To understand human nutrition it is necessary to know the nutrient requirements and to understand the function of food and nutrients in promoting and maintaining growth, health, activity and reproduction. An understanding of nutrient functions is particularly relevant in the prevention and control of nutrient deficiency diseases and protein-energy malnutrition (PEM) (see Chapter 8).
Most animal species require a number of essential dietary factors which can be classified under chemical groupings such as carbohydrates, proteins, tats, vitamins and minerals. Dietary fibre and water are sometimes added to this list. A simple classification of dietary constituents is given in Table 39. Vitamins and minerals may also be described as micronutrients. A healthy diet supplies adequate but not excessive quantities of all these nutrients. Personal requirements vary depending on individual body size, age, sex, physiological status and lifestyle.
Table 39 - Simple classification of dietary constituents
Constituent |
Use |
Water |
To provide body fluid and to help regulate body temperature |
Carbohydrates |
As fuel for energy for body heat and work |
Fats |
As fuel for energy and essential fatty acids |
Proteins |
For growth and repair |
Minerals |
For developing body tissues and for metabolic processes and protection |
Vitamins |
For metabolic processes and protection |
Indigestible and unabsorbable particles including fibre |
To form a vehicle for other nutrients, add bulk to the diet, provide a habitat for bacterial flora and assist proper elimination of refuse |
Source: FAO, 1997a.
Nutrients as energy sources
Some nutrients are interchangeable for meeting certain of the body's needs, depending on the metabolic state of the body. Carbohydrates are often divided into starches and sugars, which are both classified as "energy sources". Fats are also very concentrated sources of energy, as is clear to any fanner who includes sunflower seed, groundnut cake or soybean meal in livestock rations. Protein may also be converted into energy if the body is starved of food, but this is an inefficient use of protein. Therefore, nutritionists normally classify only starches, sugars and fats as energy foods.
Fibre, especially in the form of cellulose, is not digested in the same way as other nutrients. Most fibre stays in the gut to facilitate the digestive and excretory processes and subsequently passes out of the body in the faeces. Soluble fibre, of which there is little, ferments in the large intestine and produces fatty acids and other substances which the body absorbs and uses for energy.
Starchy staples
For most African populations carbohydrates supply most of the energy needed by the body. They yield 4 kcal per gram on complete oxidation. When carbohydrate is synthesized in a green plant, much of it is stored in the plant cells as cellulose, starch or sugar. Food crops, including grains, roots, tubers and plantains, are therefore the major sources of energy for most people in Africa and have the highest yield of energy per unit of land.
Because the body tissues require a constant supply of glucose to fuel most metabolic reactions, the digestive process eventually converts all carbohydrates (except those that make up dietary fibre) to three simple forms of sugar: glucose, fructose and galactose. The latter two are finally converted to glucose. Carbohydrates also make an essential contribution to the effective conversion and use of other nutrients, through the energy they supply. For optimum utilization of proteins, for example, carbohydrates must be supplied simultaneously, i.e. in the same meal. Similarly, carbohydrates are necessary for normal fat metabolism. The traditional African meal pattern, i.e. a carbohydrate staple complemented by relishes containing a variety of other foodstuffs, is therefore a good basis for a nutrient-efficient diet.
Starchy staples are generally eaten in larger quantity than any other dietary component in African meals. Although such foods as cereals, roots and tubers are mainly sources of energy, they also contain other nutrients, including a significant quantity of protein, especially in the case of cereals. Cereal grains are about 10 percent protein on a dry matter basis, whereas roots and tubers contain much less protein, about 1 to 3 percent (see Table 22 in Chapter 5). Legumes and oilseeds also contribute energy to the diet, from their carbohydrate and oil content; they may be 20 to 30 percent protein. When enough staple food is available to meet people's energy requirements, their protein requirements are also likely to be met. Conversely, protein undernutrition is usually associated with energy deficiency resulting from an insufficient overall intake of food. Dietary protein deficiency on its own is therefore fairly uncommon, except in circumstances where children are weaned on to non-cereal staples.
Fats and oils
Fats and oils are concentrated forms of energy. The energy yield from the complete oxidation of fatty acids is about 9 kcal per gram, in comparison with about 4 kcal per gram for carbohydrates and proteins. In addition, fats are stored in a nearly anhydrous form; animal fats contain only a small proportion of water, while refined oils contain virtually no water. People store energy in their bodies for future use in the form of fat. Some plants, in addition to storing energy as carbohydrate, also store oil in their nuts, seeds, seed germs and fruits. In Africa, much of the fat content of traditional diets comes from plant oils such as red palm oil, groundnut oil, coconut oil and sesame oil. Whole-grain cereals also contribute oil to the diet, but much of the oil may be lost if the cereal germ is separated before milling. For example, the oil content of maize drops from 4.5 percent in the dried whole grain to as low as 0.8 percent in degermed maize grits after milling.
Fats occur in foods mainly as triglycerides, which are fatty acid esters of glycerol. Fats are mixtures of various triglycerides; no fat found in nature consists of a single triglyceride. In the body, each triglyceride is broken down into glycerol and three fatty acids, all of which play a major part in energy metabolism. Over 40 fatty acids are found in nature. Naturally occurring fatty acids are classified into three groups: saturated, mono-unsaturated (with one double bond) and polyunsaturated (with two or more double bonds). The degree of saturation of any fat affects its physical and biological properties. Fats containing mainly saturated fatty acids are solid at room temperature, while those with a high proportion of unsaturated fatty acids are liquid, i.e. they are oils.
During periods of light or moderate work carbohydrates are generally a sufficient energy source. However, during extended periods of energy expenditure the body will need to use fat as an energy source once the carbohydrates have been exhausted. It is also necessary to have a certain proportion of fat in the diet to ensure an adequate energy density. It is particularly important to add small quantities of oil to weaning foods and to the diets of young children to increase the energy density of bulky foods such as cereal flours and roots and tubers.
There are other nutritional reasons to include fats in a well-balanced diet. Dietary fats are carriers of essential fatty acids and of the fat-soluble vitamins A, D, E and K. Fats also aid in the absorption of these vitamins and transport them and their precursors around the body. Fats enhance the taste of food, and they take longer to digest in the stomach than carbohydrates or proteins. They prolong the satisfaction of a meal, thus causing a delay in the onset of hunger. In addition to providing energy, tats are the building blocks of phospholipids and glycolipids, which are essential components of cell membranes.
The dietary intake of fats and oils in African meals tends to be low, as refined oils and animal foods which are sources of fats are expensive. A recent study showed that the fat consumption of women in Swaziland over a complete farming season averaged only 25 g per day, or 14 percent of their total intake of food energy (Huss-Ashmore and Curry, 1991). A general guideline for most active adults is that from 15 to 35 percent of dietary energy intake should be supplied by fats or oils and not more than 10 percent of this energy should come from saturated fat, whether derived from animal or vegetable sources. Women of child-bearing age should obtain at least 20 percent of their energy from fats to encourage adequate utilization of essential fatty acids. During weaning and at least until two years of age, children should obtain 30 to 40 percent of their dietary energy from fat, and their diet should provide about the same levels of essential fatty acids as are found in breastmilk (FAO/WHO, 1994). It would be difficult for households that do not consume enough tat to follow these guidelines. Concerted efforts must be made to ensure adequate consumption of fat among populations where less than 15 percent of the dietary energy supply is from fat. Annex 5 gives national indexes of dietary fat supplies in sub-Saharan Africa.
Essential amino acids and complementary proteins
Proteins have a crucial role in virtually all biological processes. Proteins are very large molecules made up of many amino acids linked together in different sequences. Of the large number of amino acids, 20 are common in plants and animals and are known to have a role in human nutrition. All proteins in all species, from bacteria to humans, are constructed from these amino acids, in different combinations. Nine of these amino acids are known as essential amino acids because the human body cannot synthesize them. Thus the required amounts of these amino acids must be obtained from the diet. The other 11 amino acids are also needed by the body but are considered non-essential because the human body is able to synthesize sufficient amounts of them. The relative proportions of the various essential amino acids in animal foods such as meat, fish, eggs and milk are very similar to those in human proteins, but plant proteins have them in different proportions. Proteins contain hundreds of linked amino acids, and each protein has a unique, precisely defined amino acid sequence which is genetically determined.
Proteins are the major components of muscle. The protein collagen is responsible for the high tensile strength of skin and bone. The control of growth and of cell differentiation is also a function of proteins. In the immune system, highly specific proteins - antibodies - recognize and combat foreign cells including bacteria and viruses. The response of nerve cells to specific stimuli is linked through receptor proteins, which are triggered to transmit nerve impulses at junctions between the nerve cells. In the blood, the protein molecule haemoglobin transports oxygen and carbon dioxide, while the related protein myoglobin transports oxygen in muscle tissues. Proteins include enzymes and are also essential components of body secretions and fluids such as hormones, milk and semen. Plasma proteins of the blood, particularly albumin, are important in the maintenance of the normal osmotic balance among the various body fluids.
Proteins also serve as a secondary source of energy when amounts of carbohydrates and fat in the diet are inadequate to provide sufficient energy. Thus a child given a diet with adequate protein but with intake levels below his or her energy needs will not derive full benefits for growth from the protein, but will use it as an energy source.
During digestion, dietary proteins are broken down into polypeptides and peptides and finally into amino acids, which are then reassembled to make the many different types of protein required by the body. The body uses the amino acids in making growth tissue and in repairing worn-out cells and injured tissue. Thus there is an increased requirement for protein in the diet during periods of rapid growth such as infancy, childhood and adolescence, as well as during pregnancy and lactation and during convalescence.
Proteins from animal sources contain almost the same proportions of each essential amino acid as human protein. Therefore the synthesis of human protein from animal protein is relatively straightforward. However, proteins do not all have the same value in supporting growth. Depending on the balance of their component amino acids, some have higher quality than others. Protein quality indexes, such as net protein utilization or amino acid score (see Box 53 for a definition of these and related terms), are estimates of the percentage of the total protein that can be expected to be utilized for growth and maintenance in a young animal or child. The efficiency of the protein in animal foods, including meat, fish, eggs and milk, is close to 100 percent. A food or a diet with a protein quality of 70 percent will evidently contribute more of its amino acids to growth than one with protein quality of 40 percent. However, the amino acids that are not used for protein metabolism will not be wasted; rather, they will be diverted for use as an energy source.
Proteins in plants often contain much smaller amounts of one or more essential amino acids than animal and human proteins. For example, bean protein has less methionine and maize protein has less lysine than egg or human protein. However, if maize and beans are eaten together in the same meal, the mix of amino acids produced for use in the body is improved (see Figure 27). This response has served as a basis for the formulation of high-quality-protein food mixtures containing 70 percent maize and 30 percent common beans.
Thus the nutritional quality of a meal can be maximized by combining different but complementary protein sources in the right proportions. This concept is already familiar to animal nutritionists who are engaged in balancing rations for the most effective growth of their stock animals, at the lowest cost, by using a variety of plant products. Indeed, the animal feed industry in the developed world is based on computerized mixes of complementary proteins, combined with energy foods and topped up with minerals and vitamins. Some of the principles of animal nutrition also apply to human nutrition, although components of the diets of humans and animals may differ, as their enzyme systems and the bacteria in their digestive systems differ. In any practical situation, it is necessary to assess whether the quantity of protein eaten, in conjunction with the balance of amino acids, i.e. the protein quality, is such that the requirements of the consumer for most of the limiting amino acids are met. Most evidence appears to show that although cereals are limited in protein quality by their content of certain amino acids (mainly lysine, threonine and tryptophan), conventional varieties of most cereals, if consumed in sufficient quantities to meet energy and total protein needs, contain enough of these amino acids to meet the protein requirements of preschool children. However, given the children's high requirements for both protein and energy, it is difficult for them to eat enough cereals to meet their needs. Their diets should be complemented with additional energy sources and high-protein foods such as meat, dairy products and legumes.
Box 53 - Definition of terms used in evaluating protein quality Amino acid score It the composition of an "ideal" protein - i.e. one containing all the essential amino acids in amounts sufficient to meet requirements without excess - were known, it should then be possible to compute the nutritional quality of a protein or mixture of proteins by calculating the deficit of each essential amino acid below the amount in the "ideal" protein. This approach forms the basis of the so-called amino acid scoring procedure, by which one can evaluate the capacity of a given protein or mixture of proteins to meet the essential amino acid require" meets. An amino acid score can be calculated according to the most limiting amino acid. Limiting amino acid The limiting amino acid is the amino acid in greatest deficit for the age group whose protein requirements are to be met. Only four essential amino acids are likely to limit the protein quality of mixed human diets: lysine, the sulphur-containing amino acids (methionine plus cystine), threonine and tryptophan. Digestibility of protein Large intakes of dietary fibre (e.g. cereal bran) increase the excretion of nitrogen in the faeces, reducing apparent protein digestibility by about 10 percent. Thus the overall composition of the diet must be taken into account when assessing digestibility. Protein efficiency ratio The simplest method for determining nutritive value is to measure the growth rate of young animals fed on test food. The weight gain is then related to the amount of protein eaten. The index obtained is called the protein efficiency ratio (PER). This ratio varies with the level of protein in the diet. The conventional level of 10 percent dietary protein was in general use, but the official standardized level is 9.09 percent protein. Biological value The biological value (BV) of a protein is the proportion of the absorbed nitrogen that is retained for maintenance and/or growth. It is calculated from an analysis of nitrogen intake in the diet and nitrogen output in the urine and faeces. Net protein utilization The net protein utilization (NPU) of a protein is the product of the biological value and the digestibility of a protein, i.e. the proportion of ingested nitrogen that is retained in the body under specified conditions. NPU is a combined measure of digestibility and the efficiency of utilization of the absorbed amino acids. |
Source: WHO, 1985. |
FIGURE 27 - Protein efficiency ratio of combinations of common or opaque-2 maize and black beans
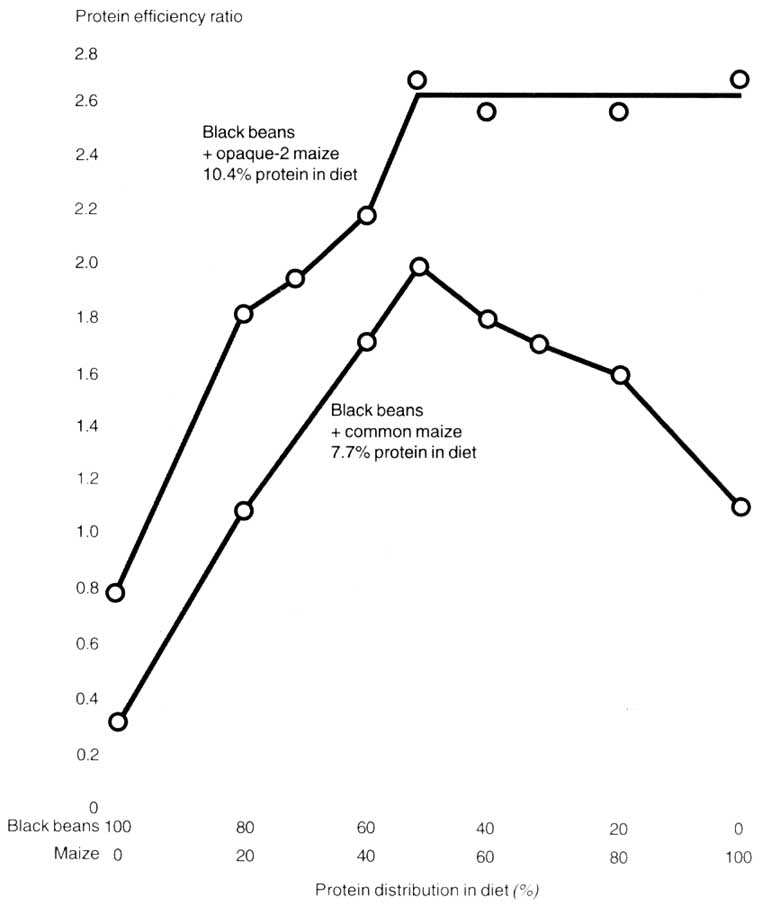
Source: FAO, 1992i (reproduced from Bressani, 1988).
In Chapter 5 the concept of complementary proteins was related to patterns of intercropping in mixed farming systems. Household production of cereal crops together with legumes provides a nutritionally effective mix of complementary proteins for the household diet, especially when the cereals and legumes are supplemented with vegetables from a home garden or with gathered leafy vegetables (FAO, 1992i).
The protein content of different foods can be compared using food composition tables such as those shown in Table 40 and Annex 4. Such tables do not indicate the amino acid score of the protein or the proportion of it utilized in the human body, i.e. the protein quality. However, they are still useful in assessing the nutritional value of foods and diets.
Assessment of protein quality and the biological utilization of proteins
Nutritionists have traditionally used experimental animals, usually rats, to assess the protein efficiency ratio and net protein utilization of different food proteins. Assessment tests, however, are usually conducted at levels of protein intake that are below the optimum for maximum growth. Figure 28 shows that the biological value of egg protein is at a maximum, around 100 percent, at an intake of 0.2 g per kilogram per day. If this intake is doubled to 0.4 g per kilogram per day the biological value falls to about 60 percent. This study shows that utilization of the protein depends on the level of feeding; beyond the level of feeding corresponding to maximum utilization of protein, any excess goes to waste.
Table 40 - Approximate composition of some cooked foodsa
Cooked foodb |
Water |
Energy |
Protein |
Iron |
Vitamin Ac |
Vitamin Cc |
Maize, stiff porridge |
75 |
100 |
2.3 |
0.3 |
0 |
0 |
Maize, thin porridge |
87 |
50 |
1.4 |
0.2 |
0 |
0 |
Rice, polished, boiled |
70 |
123 |
2.8 |
0.3 |
0 |
0 |
Rice, parboiled, boiled |
65 |
134 |
2.8 |
0.7 |
0 |
0 |
Pasta, boiled |
66 |
134 |
4.7 |
1.2 |
0 |
0 |
Cassava, fresh, boiled |
60 |
140 |
1.2 |
1.5 |
- |
0 |
Gari (fermented, dried, pounded cassava), boiled |
70 |
121 |
0.3 |
? |
0 |
0 |
Plantain, cooked |
70 |
111 |
0.8 |
0.9 |
110 |
12 |
Potato, boiled |
78 |
75 |
1.7 |
1.7 |
- |
16 |
Potato, fried/chips |
47 |
250-562d |
3.8 |
0,9 |
0 |
15 |
Sweet potato boiled |
69 |
121 |
1.6 |
2.9 |
440 |
28 |
Beans/peas, boiled |
65 |
128 |
8.8 |
3.3 |
- |
0 |
Groundnuts, boiled |
49 |
314 |
13.8 |
2.1 |
- |
0 |
Groundnuts, roasted |
4 |
585 |
25.6 |
? |
0 |
0 |
Soybean, boiled |
51 |
223 |
20.9 |
3 4 |
- |
0 |
Medium green leaves, boiled and drained |
48 |
160 |
11.5 |
? |
1 000 |
58 |
Cabbage, boiled |
93 |
23 |
1.6 |
? |
40 |
40 |
Chicken, boiled (% EP = 67) |
61 |
203 |
26.0 |
1.5 |
110 |
0 |
Fish, boiled or steamed (% EP = 52) |
74 |
118 |
20.0 |
1.8 |
- |
0 |
Source: King and Burgess, 1993.
a Calculated from values for raw foods, allowing for different water content; allowance made for some loss of vitamins during cooking.
b Percentage edible portion (% EP) = 100 unless stated otherwise.
c Content varies with the cooking method. RE = retinol equivalent.
d Varies according to how the chips are prepared.
FIGURE 28 - Biological value of egg protein at different levels of protein intake in young adult men
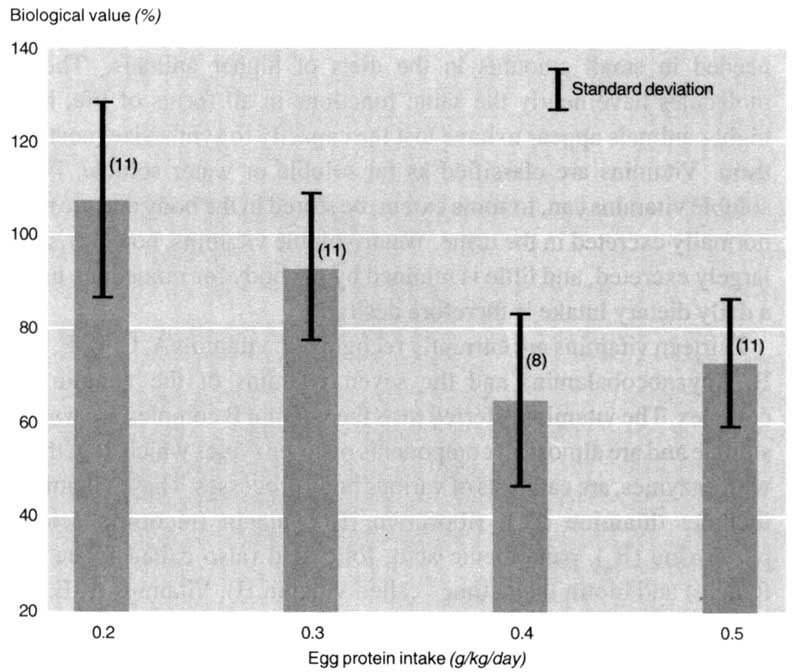
Source: Pellet and Young, 1980
Another factor that affects human utilization of protein is the amount of other nutrients in the diet. If the diet contains insufficient carbohydrate or fat to meet energy needs, the protein in the diet will be converted into energy to make up the deficit. The result is a wasteful use of an expensive nutrient. The amount of fibre in a meal may also adversely affect the digestibility of the proteins present and hence lower their biological availability.
The basic lesson mentioned at the beginning of this chapter, "eat a variety of foods", can be used to promote good intakes of complementary protein and the addition of high-energy foods to the basic staples.
Vitamins are a chemically unrelated group of organic molecules needed in small amounts in the diets of higher animals. These molecules have nearly the same functions in all forms of life, but higher animals appear to have lost the capacity to synthesize most of them. Vitamins are classified as fat soluble or water soluble. Fat-soluble vitamins can, to some extent, be stored in the body and are not normally excreted in the urine. Water-soluble vitamins, however, are largely excreted, and little is retained by the body for immediate use; a daily dietary intake is therefore desirable.
Thirteen vitamins are currently recognized: vitamins A, C, D, E, K, B12 (cyanocobalamin) and the seven vitamins of the vitamin B complex. The vitamins referred to as the vitamin B complex are water soluble and are almost all components of co-enzymes which, together with enzymes, are catalysts of various body processes. These vitamins include: thiamine (B1), riboflavin (B2), niacin (nicotinic acid), pyridoxine (B6), pantothenic acid, folic acid (also called folate or folacin) and biotin (sometimes called vitamin H). Vitamins A, E, K and D are fat soluble. Each vitamin is present in many different foods (see Table 41). Vitamin D is produced in the skin when it is exposed to sunlight, and niacin is made by the body from tryptophan, one of the essential amino acids.
Table 41 - Vitamins and main food sources
Vitamin |
Good sources |
Fat -soluble | |
Vitamin A |
Liver, fish-liver oils, egg yolk, milk and dairy products, green leafy vegetables (especially kale, amaranth, sweet potato, cowpea and cassava leaves), yellow- and orange-coloured fruits and vegetables (carrots, pumpkin, mango, papaya, oranges), orange-coloured sweet potato, palm oil |
Vitamin D |
Cod-liver oil, oily fish, liver, egg yolk |
Vitamin E |
Vegetable oils (such as maize, soybean and sunflower oils), nuts, soybeans, cereals, egg yolk |
Vitamin K |
Green leafy vegetables, vegetable oils, egg yolk, beef, mutton, poultry |
Water-soluble | |
Thiamine (vitamin B1) |
Millets, sorghum, wheat, maize, dried beans, rice, liver, kidney, beet, nuts |
Riboflavin (vitamin B2) |
Green leafy vegetables, liver, kidney, milk, cheese, eggs, whole grains |
Niacin (nicotinic acid and nicotinamide) |
Lean meat, poultry, fish, groundnuts, dried beans, wheat, yam, potato |
Pantothenic acid |
Kidney, fish, egg yolk, most vegetables, most cereals |
Pyridoxine (vitamin B6) |
Meat, poultry, fish, egg yolk, whole grains, banana, potato, dried beans, lentils, chickpeas |
Biotin (vitamin H) |
Groundnuts, dried beans, egg yolk, mushrooms, banana, grapefruit, watermelon |
Folic acid |
Green leafy vegetables (losses from cooking can be high), fresh fruits (especially orange juice), dried beans, peas, nuts, egg yolk, mushrooms, banana, liver |
Vitamin B12 (cyanocobalamin) |
Liver, kidney, chicken, beef, fish, eggs, milk, cheese |
Vitamin C |
Citrus fruits, guava, baobab, mango, papaya, green leafy vegetables, green chili, potato, green peppers, tomatoes |
Not all of the vitamins present in food are available in an absorbable form. For example, most of the niacin in cereals is bound in such a way that it is not absorbed from the gut. Fat-soluble vitamins also may not be absorbed if the digestion of fat is impaired. For example, children with diarrhoea or other gut infections, including worms, absorb less vitamin A than normal.
Minerals are another group of chemical compounds used by the body that must be provided by the diet Minerals occur in varying quantities within the food system. Some of them, such as calcium and iron, are often, like vitamins, found in a bound form and are thus not easily absorbed from the human gut. Most minerals are required in minute amounts and have very specific functions in the human body. To be discussed here are those whose deficiencies tend to precipitate a disease, for example iron and anaemia.
Vitamin A in foods and Its role in the body
Vitamin A activity in foods can occur in two forms: retinol (already formed vitamin A), which is colourless and found only in animal products, and carotene (provitamin A), which is an orange pigment found in many foods including red palm oil, carrots, sweet potato, tomato, oranges, mango, papaya and dark-green leafy vegetables (e.g. kale and leaves of cassava, sweet potato and amaranth). Carotene is converted to retinol in the walls of the intestine. There are several forms of carotene, but the most important is beta-carotene. Six molecules of carotene provide the nutritional equivalent of one molecule of retinol. Fat, protein, zinc and vitamin E all help in absorption and utilization of vitamin A by the body.
The concentration of vitamin A in foods is measured as retinol equivalents (RE) in micrograms (µg), where 1 RE = 1 µg of retinol or 6 µg of beta-carotene. Sometimes international units (IU) are used to express vitamin A concentration; 1 µg = 3.3 IU. When food tables are used to calculate values for retinol equivalents, it should be noted that vitamin A and carotene are often overestimated, since they are often determined by methods that do not separate beta-carotenes from other biologically less active or inactive carotenoids.
Vitamin A is involved in vision, as it helps to keep the front of the eye (the conjunctive and the cornea) strong, clear and moist. It is also involved in cell differentiation, reproduction and growth and in the immune response. It helps to keep all the cells on the surface of the body (epithelial cells) in a healthy condition, so that it is difficult for microorganisms to enter the body. These body surfaces include the skin, the surface of the eye, the inside of the mouth, the cells that line the gut and the cells that line the respiratory tract. When there is a deficiency of vitamin A in the body, symptoms show in the eyes and in the surface tissues.
Xerophthalmia is an eye condition in which the conjunctive and cornea become abnormally dry. Without treatment, xerophthalmia may progress to keratomalacia, a condition in which there is severe damage to the cornea, which becomes opaque and ulcerated. This condition can lead to blindness, and 50 to 80 percent of untreated children who become blind because of vitamin A deficiency usually die within a few months of becoming blind. The main determinant of mortality is their initial nutritional status.
Vitamin A also has an important role in reducing sickness and death from respiratory and diarrhoeal diseases, especially in young children. Its effect is particularly significant in cases of measles, a common disease of childhood which is still not adequately controlled in Africa.
Daily vitamin A needs for different sex and age groups are shown in Table 42. Amounts of different foods that contain approximately 500 RE of vitamin A, a quantity close to the recommended daily intake for adults, are shown in Figure 29. Fresh red palm oil is one of the richest sources of vitamin A in African diets.
Vitamin A deficiency is a serious public health problem in many countries, and its elimination is a high priority for many governments and international agencies. In this endeavour the importance of the agriculture sector, including fisheries and forestry, is paramount, as it is now generally recognized that food-based strategies offer the only safe, sustainable approach to overcoming vitamin A deficiency (and indeed micronutrient malnutrition in general, iodine deficiency being the only exception). In countries or areas where vitamin A deficiency is a problem, agricultural production policies need to be developed to encourage the increased production, processing, marketing and consumption of vitamin A-rich foods. Attention should also be given to production in household vegetable gardens and fruit orchards and in school and community gardens, as well as to commercial farming of micronutrient-rich vegetable and tree crops (see also Chapter 5).
Table 42 - Estimated daily requirements for some vitamins
Group/age |
Vitamin A |
Thiamine |
Riboflavin |
Niacin |
Folate |
Vitamin C |
Children (both sexes) | ||||||
0-6 months |
350 |
-a |
- |
- |
19 |
20 |
6-12months |
350 |
0.3 |
0.5 |
5.4 |
32 |
20 |
1-3 years |
400 |
0.5 |
0.8 |
9.0 |
40 |
20 |
3-5 |
400 |
0.7 |
1.0 |
10.5 |
53 |
20 |
5-7 |
400 |
0.8 |
1.1 |
12.1 |
65 |
20 |
7-10 |
400 |
0.9 |
1.3 |
14.5 |
85 |
20 |
Boys | ||||||
10-12 |
500 |
1.0 |
1.6 |
17.2 |
110 |
20 |
12-14 |
600 |
1.2 |
1.7 |
19.1 |
140 |
30 |
14-16 |
600 |
1.2 |
1.8 |
19.7 |
180 |
30 |
16-18 |
600 |
1.2 |
1.8 |
20.3 |
200 |
30 |
Girls | ||||||
10-12 |
500 |
0.9 |
1.4 |
15.5 |
120 |
20 |
12-14 |
600 |
1.0 |
1.5 |
16.4 |
150 |
30 |
14-16 |
550 |
1.0 |
1.5 |
15.8 |
170 |
30 |
16-18 |
500 |
0.9 |
1.4 |
15.2 |
170 |
30 |
If pregnant |
600 |
1.0 |
1.6 |
17.5 |
400 |
50 |
Men, active | ||||||
18-60 |
600 |
1.2 |
1.8 |
19.8 |
200 |
30 |
>60 |
600 |
1.2 |
1.8 |
19.8 |
200 |
30 |
Women, active | ||||||
Child-bearing age |
500 |
0.9 |
1.3 |
14.5 |
170 |
30 |
Pregnant |
600 |
1.0 |
1.5 |
16.8 |
400 |
50 |
Lactating |
850 |
1.1 |
1.7 |
18.2 |
270 |
50 |
>60 |
500 |
0.9 |
1.3 |
14.5 |
170 |
30 |
Sources: FAO, 1988b; FAO/WHO, 1974.
a -: No value available: it is assumed that breastmilk covers needs.
FIGURE 29 - Amounts of different foods that contain approximately 500 RE vitamin A (roughly the recommended daily intake of vitamin A for an adult)
Source: King and Burgess, 1993.
Vitamin D and its function in metabolism
Vitamin D has an essential role in the control of calcium and phosphorus metabolism. It helps to control the level of calcium in the blood and the amounts absorbed from the diet, deposited in the skeletal tissue and excreted through the kidneys. A deficiency of vitamin D causes a condition of bone deformities called rickets in children and osteomalacia in adults. Vitamin D is derived from cholesterol by the action of sunlight, and vitamin D deficiency is not common in Africa, where the skin is normally exposed to strong sunlight. Food sources of this vitamin are limited, and the amounts contained are variable. Vitamin D is found in whole milk, cream, butter and cheese. There is some in the flesh of fatty fish and in eggs, but these foods are perishable and expensive. Most children get all the vitamin D they need from the action of the sun on their skin, but women who live in seclusion and cover their bodies completely when outside the home may need an increased intake from their diet.
Other fat-soluble vitamins and their functions
The other fat-soluble vitamins are vitamins E and K. Vitamin E is found in all cell membranes in the body, and it is believed that there it prevents the oxidation, by molecular oxygen, of polyunsaturated fatty acids. This action is similar to that of many anti-oxidants used in the food industry to protect fats from rancidity. Vitamin E is also essential for normal cell structure, for maintaining the activities of some enzymes and for the formation of red blood cells. This vitamin also protects the lungs, the heart and other tissues from damage and helps to prevent red blood cells from being destroyed. In addition, it is believed to reduce the rate of cell ageing. A deficiency of vitamin E causes sterility in rats and can lead to spontaneous abortion in pregnant women.
The principal dietary sources of vitamin E are vegetable oils, nuts, meat, green leafy vegetables, cereals, wheat germ and egg yolk. In view of its wide distribution in foods it is unlikely that dietary shortages of this vitamin will arise. Deficiency usually occurs only through impaired intestinal absorption and is clinically manifest as anaemia. However, the most likely cause of dietary anaemia is a deficiency of iron.
Vitamin K, like vitamin A, exists in two forms. Vitamin K, is found in plants, and vitamin K2 is produced by many species of bacteria, including Escherichia coli, which inhabits the human large intestine. It is often assumed that this biosynthesis in the gut provides for the vitamin needs of the body, which would explain why human beings, with the exception of newborn infants, appear not to depend on their diet for the supply of vitamin K. Vitamin K is found in green leafy vegetables, egg yolk, vegetable oils, cheese and liver. Dietary deficiency is rare, but a shortage may arise from malabsorption during certain liver disorders or chronic diarrhoea. One of the functions of vitamin K is to facilitate blood clotting in open wounds.
The water-soluble vitamins
The water-soluble vitamins include vitamins C and B12, together with the seven vitamins of the vitamin B complex.
Vitamin C is also known by its chemical name, ascorbic acid. It was the first of the vitamins to be isolated and synthesized. Chemically it is a simple sugar, and it is the most active reducing agent known to occur naturally in living tissue. Its exact biological action in the body is not fully understood.
Vitamin C is important for the growth and maintenance of healthy bones, teeth, gums, ligaments and blood vessels. It is also involved in the production of chemicals responsible for the transmission of nerve impulses between nerve cells (neurotransmitters) and in the production of adrenal gland hormones, including the corticosteroids. Hydrocortisone, the most important of the human corticosteroids, controls the body's use of fats, proteins and carbohydrates.
Vitamin C is also involved in the response of the immune system to infection and in wound healing. In addition, it assists in the absorption by the body of non-haem iron, the form of dietary iron found in plants, eggs and milk, which is not easily absorbed through the gut wall. Citrus fruit, for example, which contains vitamin C together with citric acid, increases the percentage of non-haem iron absorbed from a meal of maize and beans or other cereal and legume mixture, as long as these are eaten at the same time.
Prolonged deficiency of vitamin C in the diet causes scurvy, a disease in which the body's immune system is weakened. The epithelial cells lose their binding power, which makes wound healing difficult and bruising easy.
The principal dietary sources of vitamin C are fresh fruits and vegetables, especially citrus fruits, guava, baobab fruits, papaya, mango, tomato, peppers, green chili, fresh animal milk and breastmilk. Vitamin C is extremely labile and is easily destroyed by heat and air. Considerable amounts of vitamin C are therefore lost if the fruits and vegetables are processed or are kept warm after cooking. Drying of fruits and vegetables also often destroys much of their vitamin C (see Chapter 6 on food storage and processing).
The most important vitamins of the vitamin B complex are thiamine, riboflavin and niacin. The main functions of these water-soluble vitamins are in the metabolism of carbohydrates during energy production and in regulating the body's use of protein.
Thiamine deficiency causes beriberi, which is not often seen today. It was associated with diets in which most of the energy came from polished rice or from highly refined flours, with very little other food. It was most common in women of child-bearing age and their children. Thiamine, riboflavin and niacin usually occur together in foods, but in different proportions depending on the food source. The richest sources are meats, fish, eggs and milk, and there are good supplies in all legumes, groundnuts and whole-grain cereals. Oilseeds have useful quantities, and small amounts are obtained from regular intake of fruits and green leafy vegetables.
A deficiency of riboflavin is more likely to occur than a deficiency of thiamine because sources of the former are more limited. Particularly good sources are liver and milk, eggs, whole grains and brewer's yeast. Prolonged deficiency of riboflavin causes soreness of the tongue, cracking of the lips and corners of the mouth and certain eye disorders, including an abnormal sensitivity to bright light (photophobia).
Niacin, which consists of nicotinic acid and nicotinamide, is involved in the production of sex hormones and the maintenance of healthy skin. Niacin is present in cereals in a chemically bound form which is not absorbed by the body. Part of the niacin is liberated and becomes available when the cereal is baked. Niacin can be made in the body from tryptophan, one of the essential amino acids of protein. This synthesis can only take place when there is excess tryptophan; 60 mg of tryptophan is equivalent to 1 mg of niacin.
The principal dietary sources of niacin include liver, lean meat, poultry, fish, groundnuts and dried beans. Seasonal deficiencies occur when adult diets are based mainly on maize or sorghum, but adults may obtain additional niacin from fermented cereal-based beverages such as beer. Prolonged niacin deficiency causes pellagra, in which the parts of the skin that are exposed to the sun develop a dark, peeling rash. Some people with pellagra may also have severe diarrhoea or mental changes.
Consumption of a diversified diet provides the best safeguard against a shortage of B vitamins.
Folic acid and vitamin B12
Folic acid and vitamin B12 are considered together as a group because they are essential for normal blood formation. Red blood cells are formed in the bone marrow; their formation requires an adequate supply of nutrients including iron, amino acids, vitamin B12 and folic acid.
Folic acid (or folate) is contained in a variety of foods, particularly liver and raw dark-green leafy vegetables. During pregnancy folic acid plays an important part in foetal growth - in the development of the nervous system and in the formation of blood cells. The body stores only a little folate in the liver, and folate, unlike iron, cannot be reused when a red blood cell dies. Thus a daily intake from the diet is desirable. Folic acid is stable in acid medium but is destroyed fairly rapidly when it is heated in neutral or alkaline conditions. Food preparation can cause serious losses, especially if green leafy vegetables are treated with alkaline soda ash and boiled for long periods to soften them before consumption as is the normal practice in some communities. The form of folic acid present in animal liver is most easily absorbed. Other foods contain most of the folate as polyglutamates and are less reliable as dietary sources. The proportion of free folate is relatively high in lentils, beans and orange juice.
A varied diet that includes fresh vegetables and fruit generally provides enough folic acid for the body's needs. Mild deficiency is relatively common but can usually be corrected by increasing the daily consumption of foods containing folate. More severe deficiency may occur during pregnancy and breastfeeding, in premature or low-birth-weight babies and in people taking certain drugs, including some antimalarials.
Vitamin B12 is found only in foods of animal origin such as meat, fish and dairy products. It is absorbed from the small intestine after first combining with a chemical called "intrinsic factor", which is produced by the stomach lining. Vitamin B12 exists in most diets in greater amounts than the body requires; the excess is stored in the liver, where it can last for several years. If a person on a normal diet acquires a vitamin B12 deficiency, it results probably not from lack of the vitamin, but from an inability to absorb it. The most common cause is an inability of the stomach lining to produce intrinsic factor. The deficiency leads to pernicious anaemia which cannot be corrected by dietary improvement.
Iron and nutritional anaemia
Iron is a mineral nutrient which is essential for the formation of haemoglobin and certain enzymes in the body. Haemoglobin is the red pigment in red blood cells and is responsible for oxygen transport. Iron is also involved in the formation of myoglobin, which is the oxygen-carrying pigment in muscle cells. Iron is contained in a variety of foods such as liver, meat, cereals (especially whole grain), fish, green leafy vegetables, nuts and beans.
Red blood cells have a life span of only about four months, so the body has to replace them throughout life. The nutrients required to replace red blood cells include iron to make haemoglobin, together with folate and protein. The body can store some iron in the tissues and can also recycle some of the iron when red blood cells die. However, a continual supply of iron must be absorbed from the diet to retain health.
There are two types of iron in food, haem iron and non-haem iron. Haem iron is obtained from the blood and meat of animals, birds and fish. However, the amount of iron ascribed to the raw form of these foods in food composition tables may be misleading. Although haem iron is relatively accessible, only IS to 35 percent of all haem iron consumed in the diet is finally absorbed through the gut wall.
The iron in plants, eggs and milk is in a form called non-haem iron and is usually present as inorganic ferric complex salts. During digestion, this inorganic iron is partly reduced to the more readily absorbed ferrous form. The conversion is markedly assisted by the presence of vitamin C. However, the human body may actually absorb less than 5 percent of the non-haem iron consumed. About 10 percent of the iron in cow's milk is absorbed. However, babies absorb about 50 percent of the iron from breastmilk, even though it is non-haem iron, possibly because infants may have a more efficient absorptive mechanism for breastmilk. The supplementary iron added to some processed foods is also usually absorbed quite well. Daily iron needs for men, women, children and infants on different diets are shown in Table 43.
Other components of a meal may alter the amount of non-haem iron that is absorbed. Absorption and assimilation of non-haem iron is increased by including foods rich in vitamin C, especially fruits, which also contain citric acid. Sources of haem iron such as liver, meat, chicken or fish, eaten in the same meal, can also increase the absorption of non-haem iron. Coffee and tea contain tannins which may reduce iron absorption from foods if these beverages are taken together with meals; therefore coffee and tea are best consumed between meals.
Fermenting and germinating grains and legumes may help to increase availability of non-haem iron. Germination may also increase the level of folate in the foodgrain (see Table 44). During germination antinutritional factors such as phytates, trypsin inhibitors and haemagglutinins may be partially degraded and may thus make non-haem iron more available. Availability of phosphorus and iron usually increases, while lysine and tryptophan may be synthesized.
Table 43 - Estimated dietary requirements for iron for people on different diets
Group/age |
Iron availability of diet. | ||
High |
Medium |
Low | |
Children (both sexes) | |||
6-12 months |
7 |
11 |
21 |
1-3 years |
5 |
7 |
13 |
3-5 |
5 |
7 |
14 |
5-7 |
7 |
10 |
19 |
7-10 |
8 |
12 |
23 |
Boys | |||
10-12 |
8 |
12 |
23 |
12-14 |
12 |
18 |
36 |
14-16 |
12 |
18 |
36 |
16-18 |
8 |
11 |
23 |
Girls | |||
10-12 |
8 |
11 |
23 |
12-14 |
13 |
20 |
40 |
14-16 |
13 |
20 |
40 |
16-18 |
16 |
24 |
48 |
If pregnant |
26 |
38b |
76b |
Men, active | |||
18-60 |
8 |
11 |
23 |
>60 |
8 |
1 1 |
23 |
Women, active | |||
Child-bearing age |
16 |
24 |
48 |
Pregnantb |
26 |
38c |
76b |
Lactating |
9 |
13 |
26 |
>60 |
6 |
9 |
19 |
Source: FAO, 1988b.
a High diet contains non-haem iron + haem iron, e.g. rice and peas + fish: iron absorption about 15 percent. Medium: diet contains non-haem iron + vitamin C, e.g. rice and peas + pumpkin: iron absorption about 10 percent. Low: diet contains only non-haem iron, e.g. rice and peas; iron absorption about 5 percent.
b Iron requirements during pregnancy are an estimate of the minimum needs over the whole nine months.
c Supplements are usually needed to provide enough iron.
Table 44 - Folate content of germinated foodgrains
Germination period |
Folate content | |
Chickpea |
Finger millet | |
0 |
213 |
14 |
24 |
306 |
16 |
48 |
344 |
63 |
72 |
374 |
84 |
Source: Babu, 1976.
Iron and/or folate deficiency, leading to anaemia, is exacerbated by conditions causing regular loss of red blood cells. Malaria parasites (protozoa known as plasmodia) destroy the body's red blood cells, which may lead to haemolytic anaemia. Some of the iron released from the ruptured cells can be reused, but the body has to replace the red cells at a faster rate than usual; this condition requires a higher dietary intake of folate. Internal and external parasites, including worms, flukes, leeches, lice, ticks and mites, all satisfy their own nutritional requirements from human blood or tissues or from the host's dietary intake, thus reducing the nutrients available to the body. Hookworm, guinea worm, bilharzia (schistosomiasis) and filariasis infections may all contribute to the loss of red blood cells and subsequent development of anaemia.
Iodine and its physiological functions
Among the minerals present in the human body iodine must be considered as a trace element or micronutrient. The adult body contains 20 to 50 mg of iodine; about 8 mg of this amount is concentrated in the thyroid gland, in the hormones T3 (tri-iodothyronine) and T4 (thyroxine), which contain 64 percent iodine. The thyroid secretions determine the level of metabolism in many cells. If the secretion is deficient, as in hypothyroidism, the basal metabolic rate falls, the circulation is reduced and the whole speed of life is slowed down. A dietary shortage of iodine may lead to enlargement of the thyroid gland (goitre). Iodine deficiency in newborns can lead to cretinism, a condition characterized by mental retardation, stunted growth and coarse facial features in infants.
Endemic goitre is usually geographically determined, as it is found in areas where the soil is deficient in iodine. Food plants that grow in such soils will also be deficient in iodine. Shortages may occur in mountainous limestone areas, in floodplains and in localities where the diet does not contain any good sources of this nutrient. The amount of iodine in food depends on the amount contained in animal feed and on the availability of iodine in the soil. Foods rich in iodine include seafoods, fish, shellfish and seaweed. The addition of iodine to cooking salt (fortification) can help to increase iodine intake. Daily estimated iodine requirements are shown in Table 45.
The availability of dietary iodine in human metabolism may be reduced if the diet contains goitrogenic agents, which interfere with the metabolism of iodine and subsequent formation of the thyroid hormones. Goitrogens may be a contributory cause of iodine deficiency disease (IDD) in areas where iodine intake is low or marginal. One important goitrogen is the toxin in poorly processed bitter cassava roots or leaves. If the cassava product contains a significant amount of residual cyanide, the cyanide may react with sulphur-containing amino acids during digestion to produce thiocyanate. Thiocyanates show marked antithyroid activity. Data from animal experiments show that goitrogens occur in a wide variety of other foods, including millets, soybean, vegetables of the genus Brassica (including cabbage and turnip) and other plants of the family Cruciferae. However, there is evidence that moderate consumption of these foods does not contribute significantly to the development of IDD, as the foods are usually cooked sufficiently to inactivate their goitrogenic components.
Table 45 - Recommended daily intake of iodine
Group |
Iodine intake |
0-6 months |
40 |
6-12 months |
50 |
1-3 years |
70 |
3-7 years |
90 |
7-10 years |
120 |
10 years to adulthood |
150 |
Pregnant women |
175 |
Lactating women |
200 |
Source: WHO/UNICEF/ICCIDD, 1993.
Other mineral nutrients
Other mineral nutrients include sodium, potassium, calcium, magnesium, phosphorus, sulphur, zinc, selenium and molybdenum. Salts of sodium and potassium are widely found in foods and are also easily absorbed from the alimentary canal and from the main cations of the body fluids.
Calcium, magnesium, phosphorus and sulphur are important components of bone and other supporting tissues. The calcium content of the diet as calculated from food composition tables is not a precise index of the amount used by the consumer, as between 70 and 80 percent of the calcium in the diet is excreted in the faeces. Absorption is facilitated by the presence of vitamin D, which is essential to calcium utilization. In addition, the calcium level in the body maintains a 2:1 ratio with phosphorus, as the two minerals tend to function and to be found together within the body. The normal secretion of parathyroid hormone also aids in the absorption of calcium, as does the presence of an adequate but not excessive intake of protein in the diet. Excessive protein intake can interfere with calcium balance. Lactose or milk sugar also enhances the digestion of calcium in animals; in humans this action appears to be related to the hydrolysis of lactose by the enzyme lactase. Phytic and oxalic acids and their salts tend to inhibit calcium uptake. Growing children and pregnant and breastfeeding women require extra amounts of calcium in the diet, as they absorb and retain more calcium for the formation of new bone.
Problems related to a lifelong lack of calcium in the diet, such as osteoporosis (bone mineral loss), are increasingly being recognized in North America and northern Europe as an important contributing factor to fractures in old age, especially among women. At present there are gaps in knowledge about the incidence of fractures in many regions, including Africa. The lifelong dietary intake of many older women in developing countries may have been deficient in the components necessary to build and protect bones, and this insufficiency, combined with a lifetime of hard physical labour, is more likely to damage than to protect musculoskeletal tissue. Adequate calcium intake throughout life and regular physical activity help to prevent osteoporosis. Good sources of calcium are milk of all types including breastmilk, cheese, small fish containing bones that can be eaten, beans and peas, finger millet and dark-green leaves.
As phosphate is a major constituent of all plant and animal cells, phosphorus is present in all natural foods, and primary dietary deficiency of phosphorus is unlikely to occur in humans. Similarly, since magnesium is a component of chlorophyll, it is present in most foods, especially those of plant origin, and dietary deficiency is rare. The main dietary sources of sulphur are the sulphur-containing amino acids cysteine and methionine. The importance of the amino acids in the diet has already been discussed in the section on proteins. The vitamins thiamine and biotin (vitamin H) also contain sulphur.
Zinc, selenium and molybdenum are trace elements that have received increased attention in recent years. However, their precise functions are still not fully known. Zinc has been recognized as essential for normal growth. There is increasing evidence of zinc deficiency in developing countries and further evidence that this deficiency is an important contributor to poor growth, reduced resistance to infectious diseases, increased incidence of stillbirths and possibly impaired cognitive development. The richest sources of bioavailable zinc are flesh foods. People whose diets consist primarily of whole-grain staple foods, as is the case in many countries of Africa, risk developing zinc deficiency, not only because such diets are low in zinc, but also because the high phytate intake tends to inhibit zinc absorption from the gut. Improved food processing techniques may in the future enhance the big-availability of zinc in cereals and legumes.
Selenium deficiency occurs mainly in places where soils are selenium deficient. Selenium is believed to have an important role in the prevention of cancer and other degenerative diseases. Recent evidence also suggests that deficiency may have a role in the pathogenesis of endemic cretinism.
Molybdenum is easily absorbed from the gut. Food sources rich in molybdenum include milk and milk products, dried legumes, cereals and red meat (especially liver and kidney). Lack of molybdenum in the diet of pregnant and lactating women is believed to contribute to impaired growth and brain development of the foetus and infant.
Setting standards
An adequate and nutritionally well-balanced diet is essential for a healthy and vigorous life. The major conditions defining an adequate diet have been discussed in Chapter 3. Numerous tables setting out standards of dietary needs have been prepared by official bodies, and some countries have developed their own national standards for nutrient requirements during the life cycle.
Such standards have three main uses. First, they provide a means of assessing the adequacy of dietary intake for different sections of the community and thus help to identify vulnerable groups at risk of malnutrition. Second, standards serve as a guide for people planning large-scale feeding programmes, as in feeding centres, schools or refugee camps. Third, they are necessary for any planned food and nutrition policy at the national or international level.
For planning purposes, dietary needs are often equated with energy needs in the preparation of national food balance sheets (see Chapter 2). Dietary intake of specific nutrients is often calculated from chemical values in food composition tables. Examples of food composition tables include Table 26 (Chapter 5), Table 40 and Annex 4.
Although nutrition experts and planners think in terms of food and nutrient requirements when planning a country's food needs and a population's dietary needs, in daily life people do not think of their meals in terms of nutrients, but in terms of different cooked foods. Box 54 shows food requirements in terms of meal requirements, as frequency of eating is an important factor in nutrition, especially for young children, who have limited stomach capacity.
Limitations of food composition tables
In order to meet the nutritional needs of a community and plan adequate diets, consumption patterns need to be reviewed together with current and accurate food composition data. Food composition data are needed, for example, to evaluate the nutritional adequacy of diets and of the food supply in a country and to assess food balance sheets and food consumption surveys. In addition, nutritional considerations are becoming increasingly important in agricultural production planning. Food composition tables can assist in crop selection, development of new varieties and traditional crop trade. However, food composition tables currently in use have significant limitations, which must be recognized if they are to be used intelligently.
Calculations of the nutrient contents of food must be based not only on representative samples of the food supply but on foods as actually eaten by a population. However, sampling error is very common, as there is potential for large differences in nutrient composition depending on the variety or strain of a food, conditions of culture or husbandry, and maturity or freshness (which can influence water content, for example). Errors may also arise from the nutrient analysis methods used, for which there are, to date, no global standards.
Box 54 - The meals that different members of the family need Men need at least two mixed meals every day and some snacks. They can get enough energy from a few large meals and from bulky foods. Women need at least two mixed meals every day and some snacks. If they are pregnant or lactating, they need almost as much food as men - especially if they are also doing hard physical work. They need much more iron and folate than men, especially when they are pregnant. Old people need at least two and if possible more meals each day as they may not eat much at each meal. They need less energy than young people but about the same amount of protein and other nutrients. Women who have stopped menstruating need less iron than child-bearing women. Old people may need soft food. Adolescents need at least two large mixed meals and some snacks each day. They can eat bulky food. Boys need a lot of energy. Girls need plenty of iron. Pregnant adolescent girls are still growing so they need more food than pregnant women. School-age children need at least two to three mixed meals and some snacks each day. Children one to five years old need breastmilk until they are at least two years old. They need at least three mixed meals and two snacks each day. They cannot eat large bulky meals. It is especially important for meals to be clean and not to contain parasites or microorganisms that could cause diarrhoea or other infection. Babies six to 12 months old need breastmilk eight to ten times or more each day. They need small meals, which are not bulky, three to five times a day. Babies under six months of age need only breastmilk at least ten times each day. |
Source: King and Burgess. 1993 |
As a general rule, figures for the composition of foods that contain a high percentage of water are always uncertain. Cereal grains contain relatively little water, and therefore tables give reliable figures for most of them. Variation in the vitamin and mineral content of foods is usually much greater than the variation in energy and protein content. The differences are especially large for all vegetables and fruits, particularly for vitamin A, ascorbic acid and minerals.
Nutrient intakes calculated from food composition data do not necessarily represent nutrients actually absorbed from the gut. For minerals and vitamins, estimates of net big-availability are not incorporated in food tables because so many constituents of food may promote or inhibit absorption. Most tables currently available also provide inadequate information about amounts of fibre, trace elements, specific fatty acids, carotenoids, tocopherols and contaminants, which are subjects of great current interest. In estimating individual nutritional status and designing treatments, a combination of dietary, biochemical, clinical and anthropometric methods will continue to be necessary. However, the improvement of food composition data worldwide and their standardization across countries are under way as part of a collaborative effort by FAO, United Nations University (UNU) and other international and national organizations (FAO, 1994c).
Energy and nutrient requirements differ at different times during the life cycle from infancy to old age. Factors influencing these requirements include age, weight, sex, basal metabolic rate, level of physical activity, physiological status (for example, whether a woman is menstrual, postmenstrual, pregnant or lactating), state of physical health (for example, disease or parasitic infection or inherent weakness because of low birth weight) and the presence or absence of various food combinations in the diet.
About half the energy needed by the body is required to activate the muscles used in daily life. The rest is used up in the growth, renewal and maintenance of the body. Individual energy requirements vary widely. Some people use over three times more energy each day than others. Most of these differences are the result of differing physical activities, but there are also differences in the speed with which energy is released and utilized by the individual. The basal metabolic rate (BMR) (for definition see footnote 1 on page 20) varies from person to person and depends on a person's level of activity, body weight, age and sex (see Table 46).
The interaction of health and nutrition is of particular significance in many African countries, where parasitic infections and childhood diseases including measles and diarrhoea, together with PEM, are major causes of childhood deaths (see Table 47). These conditions may be followed, in young adulthood, by repeated episodes of fever and malaise associated with malaria, bilharzia (schistosomiasis) and filariasis, during which appetite is reduced and absorption of nutrients is impaired.
For women, early and frequent pregnancies may contribute to poor nutritional status, especially low levels of iron and folate leading to anaemia.
Seasonal food shortages may coincide with increased physical demands in the agricultural calendar. Malnourished and anaemic children and adults lack energy and initiative, are unable to study or work intensively, and generally fail to realize their full productive capacity, including their capacity to produce, process and consume more food. Thus a continuous cycle of malnutrition leading to low production leading to further malnutrition is established.
Table 46 - Basal metabolic rate (BMR) of men and women of different weights
Weight |
Men, aged: |
Women, aged: | ||||
18-<30 |
30-<60 |
>60 |
18-<30 |
30-<60 |
>60 | |
40 |
1 291 |
1 343 |
1 027 |
1 084 |
1 177 |
1 016 |
45 |
1 368 |
1 401 |
1 095 |
1 158 |
1 221 |
1 067 |
50 |
1 444 |
1 459 |
1 162 |
1 231 |
1 264 |
1 121 |
55 |
1 521 |
1 517 |
1 230 |
1 305 |
1 308 |
1 174 |
60 |
1 597 |
1 575 |
1 297 |
1 378 |
1 351 |
1 226 |
65 |
1 674 |
1 633 |
1 365 |
1 452 |
1 395 |
1 279 |
70 |
1 750 |
1 691 |
1 432 |
1 525 |
1 438 |
1 331 |
75 |
1 827 |
1 749 |
1 500 |
- |
- |
- |
80 |
1 903 |
1 807 |
1 567 |
- |
- |
- |
Source: WHO, 1985.
Table 47 - Top ten causes of deaths in paediatric wards, Mbeya Referral Hospital, Tanzania, 1985
Disease |
Number of cases |
Percentage of all deaths |
All forms of PEM |
117 |
48 |
Pneumopathies |
32 |
13 |
Isolated diarrhoea |
21 |
9 |
Measles |
17 |
7 |
Cerebral malaria |
16 |
7 |
Anaemias |
11 |
5 |
Bacteria, meningitis |
10 |
4 |
Septicaemia |
9 |
4 |
Poisonings and drug overdoses |
2 |
1 |
Congenital malformations |
2 |
1 |
Others |
7 |
3 |
Total |
244 |
100 |
Source: Mduma, 1987.
FAO has developed a methodology and computer software to calculate population energy requirements, called ENREQ2. This methodology takes account of recommended allowances for children and pregnant or lactating women, levels of physical activity for adolescents and adults, level of infection and basal metabolic rate. Database files contain demographic, weight and height data pertaining to FAO member countries with populations exceeding 300 000, permitting the calculation of human energy requirements for populations in different situations. The software offers a flexible tool for decision-makers wishing to calculate energy requirements for populations of known composition or with special characteristics, including refugee populations containing a high proportion of women and children and requiring food assistance.
Pregnancy and lactation
A woman needs extra energy and protein during pregnancy to build up her body in preparation for breastfeeding and to provide for the growing demands of the foetus. Her additional needs depend on her activity levels and on her initial state of nutrition. Well-nourished women with light to moderate activity levels should aim to increase their intake by 100 kcal and about 6 to 7 g of extra protein per day. A well-nourished woman performing heavy activity, such as subsistence farming, may need an additional 200 kcal per day. Undernourished women should increase their intake by 200 to 285 kcal per day to reduce the risk of delivering an underweight baby and to ensure a good supply of breastmilk.
A breastfeeding mother needs about 500 kcal and 18 to 21 g of extra protein each day. Energy and nutrients to make breastmilk come partly from the mother's food intake and partly from the reserve stores of nutrients that she built up before and during pregnancy. Building up good stores is more important for making breastmilk than eating more food after the baby is born.
Approximate daily energy and protein needs for pregnant and lactating women are included in Table 48. Pregnant and lactating women also need an increased supply of iron, folate and vitamins A and C to meet the increased demands made on their bodies for these nutrients.
Infancy and weaning
During infancy, breastmilk provides all the nutrients that a baby needs. If the mother's nutrition has been satisfactory, these nutrients will be present in her milk in exactly the right proportions. The nutrients in breastmilk are more easily digested and absorbed and are more efficiently used by the baby's body than those in artificial milk mixtures (bottle feeds). Breastmilk also contains living anti-infective factors which protect a baby against infection. Some of the many advantages of breastfeeding are that it helps to delay a new pregnancy, it costs less than artificial feeding and it strengthens the bond between mother and baby.
Table 48 - Daily requirements for energy and protein
Group/age |
Energy |
Protein | |
Diet Aa |
Diet Bb | ||
Children (both sexes) | |||
0-6 months |
585 |
10 |
-c |
6-12months |
960 |
14 |
- |
1-3 years |
1250 |
14 |
23 |
3-5 |
1510 |
18 |
26 |
5-7 |
1710 |
20 |
30 |
7-10 |
1880 |
26 |
38 |
Boys | |||
10-12 |
2170 |
34 |
50 |
12-14 |
2360 |
43 |
64 |
14-16 |
2620 |
52 |
75 |
16-18 |
2820 |
57 |
84 |
Girls | |||
10-12 |
1925 |
35 |
52 |
12-14 |
2040 |
42 |
62 |
1416 |
2135 |
46 |
69 |
16-18 |
2150 |
45 |
66 |
If pregnant |
+200 |
+6 |
+7 |
Men, active | |||
1 8-60 |
2 944 |
49 |
57 |
>60 |
2 060 |
49 |
57 |
Women, active | |||
Child-bearing age |
2140 |
41 |
48 |
Pregnant |
2 240 |
47 |
55 |
Lactating |
2 640 |
59 |
68 |
>60 |
1830 |
41 |
48 |
Source: WHO. 1985.
a A mixed balanced diet with little fibre and plenty of complete protein, digestibility factor 100%, amino
acid score 100 for all ages.
b A high-fibre diet containing a large amount of cereals, starchy roots and pulses and little complete
(animal) protein; digestibility factor 85%; amino acid scores 70 for ages 1 to 5 years 80 for ages 5 to
17 years and 100 for adults.
c -: No value available; it is assumed that breastmilk covers needs.
Provided that the mother's own diet is good, her baby will thrive and grow steadily on her supply of breastmilk for the first four months of life. If solid foods are introduced to the infant too early, there is a risk that the infant's demand for breastmilk will be reduced. As a consequence of this reduced demand the mother will produce less milk, and early weaning will follow. The recommended gradual weaning process goes from exclusive breastfeeding (complete dependence on breastmilk), through partial breastfeeding plus weaning foods, to token breastfeeding, when the infant is able to eat family foods and will finally give up breastfeeding altogether.
Frequent meals and a high nutrient density in the infant's diet will help to ensure a safe and successful weaning period. In order to provide a child with more frequent meals or denser weaning foods, increased care-giving time and effort are needed. A good solution is a community-based care programme developed by a group of mothers, providing care in one of their homes and staffed by one or more mothers under the guidance of a visiting supervisor. Such programmes will be more effective if they form part of an overall development programme with official assistance and government support.
School-age children and adolescent girls and boys
The foods provided for school-age children should satisfy the high demands of rapid growth, intense physical activity and mental development. Between the ages of 11 and 16 years children grow very quickly and need extra food in the form of snacks in addition to regular meals (see Box 55). Snack foods can often be quite nutritious and high in energy, especially if they are fried in oil.
Children who arrive at school in a state of hunger will not be able to concentrate on their lessons, and their learning will suffer. The provision of school breakfasts may be an appropriate intervention in this case. Research findings indicate that mild to moderate malnutrition acts synergistically with social and environmental factors to reduce the educational performance of schoolchildren (Levinger, 1989). Low energy levels lead to inactivity and short attention span; a chronic state of undernutrition will prevent a child from achieving his or her full potential, both mentally and physically.
Box 55 - Snacks for school-age children Examples of good snacks These snacks are often good value for money: · boiled, pasteurized or soured milk; · bread or chapati (fried wheat bread), especially with an energy-rich food such as margarine or groundnut paste or simsim (sesame) paste; · doughnuts, bean cakes, biscuits; · boiled or fried cassava, plantain, yam or potato (e.g. chips); · boiled or roasted maize cobs; · bananas, pawpaw, avocado, mango, oranges and other fruits; · coconut flesh; · boiled egg; · cooked groundnuts, soybeans and other oilseeds; · small fried fish; · insects such as locusts or termites; · sugar cane. Examples of poor snacks These snacks are often poor value for money, and their frequent consumption can be bad for the teeth, so they should be kept for special treats: · sodas; · sweets and follies; · ice-cream; · glucose powder and tablets; · crisps and other similar snack foods. |
Source: King and Burgess, 1993. |
Old age
As humans grow older, throughout adulthood, their need for food and nutrients declines as activity diminishes. There may also be a small reduction in the basal metabolic rate, associated with reduced cell mass. Further changes in dietary patterns may occur when illness restricts physical activity. Tables 42, 43 and 48 can be used to compare the energy and nutrient needs of women of child-bearing age and women aged over 60. Iron requirements are reduced in postmenopausal women, as they no longer experience blood loss through menstruation, and energy requirements are less when activity is limited. However, requirements for other minerals such as calcium remain the same, as do those for vitamins. If energy intake is reduced it is probable that the intake of vitamins and minerals will also suffer. It is therefore important to ensure that the diets of older people do not become too monotonous and limited. Whenever possible, they should include daily intakes of fresh vegetables and fruit and particularly those foods that supply vitamins A, C and D.
A policy of encouraging families to care for their elderly, in keeping with African cultural traditions, has tremendous advantages and imposes far less burden on national resources. Family care provides emotional satisfaction to the elderly and could prove far more conducive to the maintenance of their health, nutritional status, productivity and dignity. A good proportion of elderly people between 60 and 70 years of age can continue to function as valuable members of society. In African societies the senior members of extended families traditionally enjoy a respected position and continue to have a dominant role in family decision-making.
Relations among diet, ecology and the food supply system
In relation to nutrition, not only the composition of the diet is significant, but also the meal frequency patterns and the distribution of foods within the family. The food habits and dietary patterns of a community are often closely related to its ecological zone.
Domestication of plants, in response to natural ecosystems, has led to two main cropping systems. Seed culture (raising of crops from seeds) is the indigenous mode of agriculture in the drier regions of Africa. Root and tuber culture, dependent mainly on vegetative reproduction, is more highly developed in the humid tropical lowlands of Africa. Plant domestication can also lead to dependence on a single staple, such as rice, maize, cassava or plantain. If this staple is low in certain nutrients, nutritional deficiencies may result.
Nomadic pastoralists do not normally cultivate crops. Their traditional diets are based largely on animal products from their own herds, supplemented seasonally by a variable range of wild gathered foods in most communities. Increasingly, however, cereal products such as sorghum and millets are now included in their diets. See Chapter 4, Box 17 for a discussion of the food supply system and its nutritional consequences for a pastoral family in the Malian Sahel.
Other changes in the food supply system which are reflected in the diet are related to the increasing urbanization of African populations. Such dietary modifications include consumption of different dietary staples and an increase in the purchase of snack foods (see Chapter 3). There has been a shift away from sorghum, millets and yams towards modern foods such as maize, rice, wheat and wheat products, particularly in the cities.
Composition of African diets
Generalizations are rarely helpful in describing a subject as complex as diets, which depend on many economic, ecological, social and cultural factors and tend to be location and community specific. African diets are usually based on a carbohydrate staple served with soups, relishes and sauces, which may or may not be spicy, prepared from a wide variety of other foodstuffs. Figure 30 shows the proportions of different food groups in the consumption patterns of women and children in Swaziland.
Most of the dietary energy comes from the staple, which may also make a considerable contribution to the protein content of the meal. Staple cereals such as maize, sorghum, millets and rice contribute 40 to 60 percent of the total dietary energy supply (DES) in most countries. The relish provides oil, protein, vitamins and minerals. It makes the starchy staple more palatable and satisfies the appetite. The components and the nature of the starchy staple will remain fairly constant within a community, while the relish (usually composed of vegetables, pulses or nuts and fish or meat if available) will vary in components, flavour and consistency depending on the season, household resources and dietary habits. Few data are available on vegetable consumption in Africa, as the assessment is complicated by the fact that vegetables are obtained as wild crops.
FIGURE 30 - Composition of the diet of women and children in Swaziland:
WOMEN
CHILDREN
Source: Huss-Ashmore and Curry. 1991.
The oil or fat content of many African diets tends to be very low (see Annex 4). Total dietary fat provides on average 18 percent of total food energy in sub-Saharan Africa, but populations in some countries obtain as little as 7 to 15 percent of food energy from fat. The content of animal protein also tends to be quite low. Meat (primarily sheep and goat meat) and meat products provide an average of only 3 percent of DES. Milk is scarcely consumed in Africa (except in some countries in the Sahel such as Kenya, Mauritania, Somalia and the Sudan), because of the very low production of milk per animal and the lack of preservation technology. Another factor may be the high lactose intolerance among the population.
Given their limitations of resources and of access to different foods, most African communities have developed diets that maximize the use of local foodstuffs. Dietary deficiencies are often the result of lack of money, of resources, including labour and land, and of time, especially for women.
Table 49 shows examples of family diets that might be eaten in different localities in East Africa. They are not average diets in these areas, but suggestions for diets that would be satisfactory if the component foods are available and accessible to the family. These diets and the meals shown in Box 56 may provide guidance to extension and home economics officers who wish to advise households on feeding their families. If the household has access to land and to labour, these guidelines may also influence advice on horticultural and agricultural production for domestic consumption. In poor circumstances the most appropriate advice is probably to ensure a more equitable distribution of the available food and to improve the situation for children by encouraging breastfeeding and more frequent feeding of infants and weaning-age toddlers.
Table 49 - Dietary suggestions for daily food intake in seven localities in East Africa
Food |
Amount |
Kenya coast | |
Rice |
500 |
Fish |
100 |
Beans |
150 |
Amaranth |
100 |
Mango |
100 |
Coconut |
50 |
Oil |
15 |
Salt |
15 |
Uganda village | |
Plantains |
1 000 |
Sweet potatoes |
200 |
Meat |
50 |
Beans |
150 |
Sweet potato leaves |
150 |
Tomatoes |
50 |
Oil |
15 |
Salt |
10 |
Morogoro Region, Tanzania | |
Maize |
500 |
Dried sprats |
50 |
Cowpeas |
100 |
Amaranth |
100 |
Oranges |
100 |
Onions |
50 |
Oil |
15 |
Salt |
10 |
Nairobi, Kenya | |
White wheat-bread |
400 |
Rice |
100 |
Eggs |
30 |
Meat |
100 |
Carrots |
100 |
Green leaves |
50 |
Butter or margarine |
25 |
Fresh bananas |
100 |
Milk (in tea) |
60 |
Sugar |
30 |
Salt |
10 |
Mozambique, rural | |
Millet |
400 |
Cassava |
200 |
Sour milk |
150 |
Tomatoes |
100 |
Cassava leaves |
100 |
Groundnuts |
50 |
Bambara nuts |
75 |
Baobab fruit |
30 |
Salt |
10 |
Lake Victoria shore | |
Maize |
600 |
Fish |
100 |
Cowpeas |
150 |
Papaya |
150 |
Vegetables (mixed) |
200 |
Groundnuts |
75 |
Oil |
20 |
Salt |
10 |
Masailand (pastoralists) | |
Milk |
2 000 |
Blood (animal) |
100 |
Maize |
150 |
Wild leaves |
100 |
Wild fruit |
100 |
Bananas |
200 |
Salt |
15 |
Source: Adapted from FAO, 1979.
a Amounts given are those for an average man.
Box 56 - Family use of vegetable mixtures to improve the quality of the diet Where foods of animal origin are not often available the quality of the protein in the diet can be improved by providing a mixture or variety of vegetable products at each meal. Thus if a household has maize and beans available it is far better nutritionally to eat some of both at each meal rather than to eat maize for two weeks and then beans for two weeks. The former is frequently practiced by many people in East Africa. For example, trio, a traditional Kikuyu food, includes maize, beans, potato and green leaves, and the Kamba food isyo is a mixture of whole-kernel maize with beans and sometimes vegetables. The various foods do not have to be physically mixed together, but can just as well be eaten separately at the same meal. Examples of vegetable mixtures are given below, some of which are traditional dishes: · rice and bean stew; · beans and boiled maize (nyoyo); · maize, beans and green leafy vegetables; · baked sweet potatoes served with peas or beans and amaranth leaves; · uji or ugali made from one part cassava flour, two parts maize flour and served with sauce made from cowpeas and tomatoes; · sorghum gruel and bananas with groundnut paste; · millet served with onion, yam, peas and tomato relish; · groundnut soup with potatoes; · sesame (simsim) or groundnuts served with ugali; · vegetable stew (green leaves, tomatoes, beans and onions) served with rice or ugali; · cassava with bean mush; · plantains with beans and cabbage. |
Source: FAO, 1979. |
Frequency of meals and distribution of food within the family
Meal frequency in most households is adapted to the lifestyle and work patterns of the family. In many rural households the main family meal is prepared and served in the evening, after the adults have returned from the fields and the children have walked home from school. Breakfast often consists of reheated (or cold) leftovers from the previous day's main meal, together with tea. In urban areas bread and tea or coffee are taken at breakfast. In some cases, if the workplace or school is distant, adults or children may leave home before breakfast and carry with them some cold food to be eaten on arrival. Many children walk to school without having eaten anything.
In urban areas men and women may eat a midday meal at the workplace, purchased either from vendors or from a workers' canteen. For men living alone in rented accommodation with limited cooking facilities, this may be the main meal of the day. In the evening the men may congregate in local eating houses for snacks, roasted meat and beer. In rural areas the midday meal may be carried to the farming areas and eaten in the fields during the planting, weeding and harvesting seasons. Schoolchildren are sometimes given a small sum of money to purchase a snack at midday. Alternatively, they may contribute food or cash for a prepared meal at school if facilities and helpers are locally available to cook it.
Preschool children and infants may travel with their mothers to the farm, to the workplace (if permitted) or to the local market if the mother regularly sells or buys produce. When the child remains with the mother throughout the day, he or she is likely to be fed regularly with breastmilk and/or snacks. Small children left at home may be cared for by older siblings, grandparents or other relatives. Ensuring adequate food intake for such children is often difficult, and breastfeeding may be reduced or abandoned at an early stage when the mother faces this situation.
When family meals are eaten together, often in the evening or at weekends, the manner of serving the meal and the distribution of the different food items may markedly affect the dietary intake of different family members. In some households it is customary for everyone to eat from communal bowls. When this is the case, children are trained not to be greedy, but to give preference to their elders, especially regarding the meat content of the soup or relish. Young children may find it difficult to consume sufficient foods to meet their needs, and all children will be expected to concentrate their attention on the starchy staple until their father has been satisfied from the soup pot. In other communities, the mother will serve her husband and any adult males first. She will then join her children in eating after the men are satisfied. Sometimes male children are fed before the mother, the female children and the babies. Thus the order of feeding reflects the family's priority for feeding the main wage earners, but this may result in undernutrition for the most vulnerable members. Box 57 and Table 50 show results of a study regarding the effect of food distribution patterns on nutritional status within Nigerian families. It is important to note that although unequal distribution of foods within the household was often a problem, the main problem was usually an inadequate supply of available food.
A woman does not plan a diet in terms of nutrient requirements when she is feeding her family. Food production, processing and preparation are so much a part of a her daily life that she probably would find it difficult to say how she feeds the family. Certainly, if she is a farmer she will try to grow and store the foods that her family will enjoy and that she is used to cooking. However, her preferences in this respect may be limited by the type and area of her land, the amount of assistance she can expect from her children and the storage facilities at her disposal. If she has to purchase food, her cash income will often be the limiting factor in her choices for the family diet. Other factors may also be important. What is the fuelwood and water situation? How much time does she have in which to cook the meal? Should some of the vegetables from her home garden be set aside to sell next day in the market? These questions are all relevant to the choices of meal patterns in family cooking. Add to these concerns the breastfeeding demands of the new baby or the needs of the two-year-old for frequent, energy-dense feeds, and it is easy to understand why many women can answer the health worker's questions about the composition of balanced meals but do not conscientiously apply this knowledge to the family's diet.
Box 57 - Intrafamilial distribution of food and nutrients in a rural Nigerian population The study revealed that the young male child had preferential treatment over his female counterpart with respect to food intake, thereby pointing to discrimination in matters of diet in the young male and female child. Children up to the age of five years certainly need less energy than adults; but a six-year-old consumes the same amount of energy as a smallish moderately active adult. Teenagers consume more. Wheeler (unpublished observations) has pointed out that in poor rural households, there were differences of the order of 30 to 50 percent between energy intakes of adults and children as well as between sexes. In this study, the differences were in the order of 20 to 50 percent between energy intakes of adults and children. This could be attributed to important socio-cultural factors observed influencing food distribution in the homes, such as who was first served food. The father was served first followed by children in order of seniority. In this male-dominated society, the influence extended to who got the first choice of food; the sequence in which meals were served; and the attitude towards food which was often positive for preferred foods. Prestige foods were often reserved for men to attend to first before women and children. Most times, as observed in this study, Ibos serve a visitor more food than members of the household, showing the importance attached to hospitality in this culture. Cultural practices - for example, the intrafamilial food distribution pattern in which the adult male has priority in servings of meat and fish - may have a deleterious effect on the vulnerable groups. It is important to note that most times it was not unequal distribution of food within the households that might be the main problem, but that the available food supply was simply inadequate. In this study, the adult male was in negative nutrient balance except for iron and ascorbic acid. The implications of the study were that all members of the households were not getting enough food to eat, and some members, especially the vulnerable ones, consumed less than the FAO and WHO requirement values, which consequently led to poor nutritional status. |
Source: Okeke and Nnanyelugo, 1989. |
Table 50 - Person first served food in two Anambra State communities in Nigeria
Person |
Opi |
Odageri-edda |
Total | |||
Number |
% |
Number |
% |
Number |
% | |
Father |
132 |
86.8 |
49 |
98 |
181 |
91.9 |
Mother and children |
15 |
9.9 |
1 |
2 |
16 |
8.1 |
Oldest children |
5 |
3.3 |
- |
- |
- |
- |
Total |
152 |
100 |
50 |
100 |
197 |
100 |
Source: Okeke and Nnanyelugo, 1989.
Perhaps the most useful general rule in African family feeding is to give everyone (except babies) different amounts of the staple but the same share of the relish. As a general rule, a small amount of animal food can be added to the relish to provide a complete protein, so that even a small amount will improve the protein value of the meal. The animal food may also help to provide fat for energy, haem iron and vitamins, especially vitamin A and folate (from liver). Where foods of animal origin are not often available, the quality of the protein in the diet can be improved by providing a mixture or variety of vegetable products at each meal (see Box 56). The family may need to adjust its food habits, within the family's resources, to ensure that the food eaten by individual members matches their nutrient requirements more closely.
![]()
![]()
![]()
![]()