![]()
![]()
![]()
Contagious bovine pleuropneumonia (CBPP) is an acute, subacute or chronic mycoplasmal disease of cattle, which may cause high production losses and mortalities. It is characterized by fibrinous pneumonia, serofibrinous pleuritis, and oedema of the interlobular septa of the lungs.
CBPP is currently mainly a disease of Africa, where it is regarded as one of the most serious transboundary animal diseases. Most countries in sub-Saharan Africa are endemically infected, with at least 27 countries reporting its presence. Exceptions are a number of countries in southern Africa, including Botswana, Malawi, Mozambique, Republic of South Africa and Zimbabwe, and all but the northern border areas of Namibia. There was an upsurge in the incidence of CBPP in Africa in the 1990s and serious spread of the disease in eastern and parts of southern Africa, with re-introduction to areas that had been free for considerable periods. This culminated in introduction of CBPP to northern Botswana in 1995. It was eradicated from there by a stamping-out campaign and the country was able to declare provisional freedom in January 1997.
CBPP has been present in some Mediterranean countries of Europe during the last decade (Italy, 1993; Spain, 1994; Portugal, 1999).
The disease may still be present in parts of Asia, but this is uncertain. Bangladesh is the only country currently officially reporting its presence. The other continents are free.
CBPP is caused by Mycoplasma mycoides subsp. mycoides Small Colony variant (bovine biotype) (MmmSC for short). This is a member of the ‘mycoides cluster,’ a grouping of six closely related mycoplasmas that are all pathogenic to a greater or lesser degree in ruminants. Members of the cluster have a high degree of serological and DNA relatedness. There is only one serotype of MmmSC.
MmmSC, like other mycoplasmas, lacks a cell wall and is pleomorphic. In young cultures it tends to appear as branching filaments, and in old cultures as small coccal bodies. It requires special media rich in cholesterol (added serum) for growth.
The organism is fragile and survives poorly outside the host. It is sensitive to desiccation and disinfectants.
CBPP is mainly a disease of cattle. Both Bos taurus and Bos indicus breeds are fully susceptible. Water buffaloes have a lower level of susceptibility. The disease has also been reported in yaks and bison. Camels, wild bovids and other wild ruminants are resistant. The causative organism has been isolated from sheep and goats, but there is no evidence that these species play any part in the transmission of the disease.
The disease is transmitted almost exclusively by direct contact between infected and susceptible cattle, by means of infected aerosols from exhaled air. Airborne spread up to 200 metres is thought to be possible. Conditions under which cattle are herded closely together favour rapid spread of the disease. Asymptomatically and chronically infected animals are very important in the spread of the disease to new areas. Chronic carriers are apparently healthy animals that have a localized focus of infection sequestered in a fibrous capsule in their lungs. Such animals are often referred to as “lungers”. The organism can persist in such lesions for many months, and in time the fibrous capsule may break down, allowing viable organisms to escape by the bronchi and so infect susceptible in-contact animals. This is particularly prone to occur when chronic carrier animals are subjected to stress, such as when mustered or walked for long distances. As the mycoplasma survives poorly in the environment, indirect methods of spread (e.g. by fomites) are unimportant.
Epidemic CBPP may occur when the disease is introduced to previously free herds, areas or countries. It is characterized by a high incidence of disease in herds with a high proportion of cases being at the acute end of the clinical spectrum and many deaths. Spread of infection within and between herds may be rapid, particularly under conditions where cattle are congregated together, such as at watering points and markets and when droving or kraaling animals.
In the early stages of an outbreak, the intensity of infection may be low and the resultant spread may be slow. Under these circumstances, it may take several months for the epidemic to build up momentum. This early period is particularly dangerous in terms of early detection and disease containment.
Because of the variable and often long incubation period, and the fact that the disease may have been introduced by apparently healthy animals, it is often difficult to trace the timing and source of the disease introduction.
Unless the disease is effectively controlled, it will eventually become endemic and this is the situation that pertains in much of Africa. Endemic CBPP is characterized by insidious spread, and a high proportion of cases being at the less acute and more chronic end of the clinical spectrum. The mortality rate is low. There are occasional flare ups, and overall there are still substantial production losses in the endemic situation.
The incubation period is generally 3 to 6 weeks, but may be as long as 6 months.
In the acute form, there is fever (lasting 3 to 10 days), anorexia, loss of milk production in milking cows, severe depression, and rapid, laboured breathing, which is abdominal in nature. This is soon followed by dry coughing, which progressively becomes more severe, and apparent chest pain, with the animal typically facing into the wind with its back arched, elbows out and head extended. There may be nasal discharge, sometimes streaked with blood, and frothy saliva accumulates around the mouth. The mortality rate from acute CBPP may be up to 75%, and death usually occurs within 3 weeks of the onset of clinical signs. Animals that recover are extremely weak and emaciated. Many become chronic carriers. A hyperacute form may also occur in a few animals early in outbreaks - in this form, animals die with few premonitory signs.
Subacute and chronic cases are common. The clinical signs are milder and may not be detected. There may be an intermittent fever, some loss of condition, and respiratory signs that may become apparent only when the animal is vigorously exercised. Subclinical cases also occur.
In calves up to 6 months, CBPP may manifest itself only as arthritis, with lameness and a soft, puffy swelling of affected joints.
In acute CBPP, there is a severe fibrinous pneumonia with copious pleural exudate. The latter is a striking feature, and there may be up to 30 litres of yellow exudate, containing clots, in the chest cavity. One or both lungs may be partially or completely consolidated, giving a characteristic marbled appearance. Affected areas are swollen, vary from pink to dark red, have a moderately firm consistency, and exude clear fluid and sometimes blood from cut surfaces. The interlobular septa are grossly thickened. Pleural surfaces over affected areas are thickened, grey to red, and are often covered by friable, yellow fibrin. Local lymph nodes are enlarged, oedematous, and may contain areas of necrosis.
In chronic cases, necrotic lung tissue becomes encapsulated to form a sequestrum of 1 to 20 cm diameter. The tissue within the sequestrum [plural = sequestra] tends to retain much of the architecture of the acute lesion, but may eventually become calcified or liquefied. The lesion may either break open to release viable mycoplasmas or be resorbed. Pleural adhesions are commonly found in chronic cases.
Microscopically, the earliest pulmonary lesions consist of foci of catarrhal bronchiolitis, with distension of the lymphatics in the interlobular septa and thickened alveolar walls. At the same time, or soon after, blood vessels and lymphatics become thrombosed, and alveoli are filled with fluid and cells (alveolar macrophages and sometimes polymorphonuclear leucocytes). There is proliferation of the cells in lymphatic follicles and an increase in the population of mononuclear cells around bronchioles. There is also lymphatic oedema, with distension of subpleural lymphatics.
Necrosis can occur early and tends to have a lobular distribution. It is often demarcated from living tissue by a zone of leucocytes and nuclear debris. A connective tissue capsule develops rapidly, but the necrotic material may persist for many months.
Resolution of the pneumonia is by slow connective tissue replacement of damaged tissue. This starts around blood vessels. A layer of mononuclear cells borders the connective tissue on the necrotic side, and connective tissue gradually moves in to replace the dead tissue.
The occurrence of respiratory disease in a number of cattle in a herd (Plate 1) in which there is acute or chronic coughing, dyspnoea and loss of weight should be viewed as highly suspicious of CBPP. The cardinal respiratory signs to look for are fast, difficult and noisy breathing; discharge from the nose (Plate 2) and coughing, especially after exercise.
The gross lesions are highly characteristic. CBPP should be strongly suspected when there is yellow fluid in the chest cavity; lungs covered with yellowish material (Plate 3); lungs adhered to the chest wall; lungs that do not collapse and are solid, hepatized or marbled (Plate 4); or sequestra (Plate 5) can be seen in the lungs of chronic cases.
Plate 1. Appearance in the herd
This cow is having difficulty in breathing. It stands with its head and neck extended and legs widely placed. Often the elbows are turned out.
Inflammation of the membranes surrounding the lungs causes pain in the chest, resulting in abdominal breathing movements.
Poor general condition.
(Photograph courtesy of A. Provost)
The clinical signs and pathology of CBPP are fairly characteristic. Nevertheless, there are a number of diseases that may possibly be confused with it. These include:
rinderpest,
haemorrhagic septicaemia,
East coast fever,
bronchopneumonia resulting from bacterial or viral infections,
acute pasteurellosis,
bovine tuberculosis,
actinobacillosis,
traumatic pericarditis,
abscesses, or
hydatid cysts.
Plate 2. Typical nasal discharge in a CBPP-infected animal.
(Photograph courtesy of Veterinary Tropical Diseases Department, University of Pretoria, Republic of South Africa).
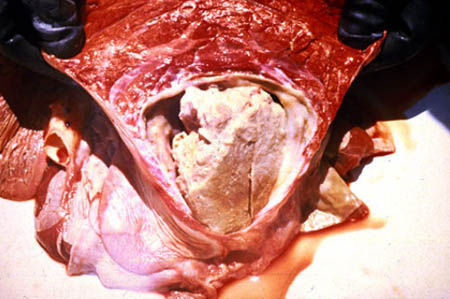
Plate 3. Characteristic post mortem appearance
Part of has been diaphragm cut away to show heavy fibrin deposits (“omelette”) on lungs and yellowish pleural fluid in chest cavity.
(Photograph courtesy of the University of Pretoria, Republic of South Africa)
Plate 4. Gross pulmonary change
Acute CBPP. Lungs cut to show red hepatization, i.e. liver-like appearance and feel to the lungs. Note the thickened interlobular septae.
(Photograph courtesy of W. Amanfu)
Plate 5. Chronic CBPP with sequestra
Sequestra are typical lesions of CBPP to be looked for during meat inspection. Chronic cases of CBPP often have such lesions.
(Photograph courtesy of R. Windsor)
Whilst histopathology helps, definitive diagnosis is based on isolation and identification of the causative agent and/or the finding of specific antigens or antibodies by appropriate serological tests.
Detailed instructions for laboratory diagnostic procedures for CBPP are to be found in the OIE Manual of Standards for Diagnostic Tests and Vaccines (4th Edition, 2000; this can be found at www.oie.int). The following is a summary, with the emphasis on the tests that are usually used.
Collection and transport of diagnostic specimens
Specimens of lung tissue from obvious lesions, tracheobronchial and mediastinal lymph nodes, and at least 10 ml of pleural fluid should be collected aseptically. Joint fluid from affected joints of calves should also be collected. Duplicate tissue specimens should be collected into neutral buffered formalin for histopathology.
Blood samples, about 20 ml each, for serum should be collected from any cattle showing clinical signs, as well as from several apparently healthy animals in the affected herd.
Unpreserved tissue, pleural and joint fluid specimens are best placed in a transport medium that will protect the mycoplasmas and prevent the proliferation of bacteria (heart infusion broth without peptone and glucose, 10% yeast extract, 20% serum, 0.3% agar, 500 IU/ml penicillin and 1:10 000 thallium acetate). These and serum specimens should be chilled and forwarded to the laboratory on water ice or with frozen gel packs.
Culture and identification of MmmSC
MmmSC can be isolated from unpreserved tissue and fluid specimens in suitable mycoplasma media such as Hayflick’s or Gourlay’s broth containing penicillin and thallium acetate. The organism is detected by regular dark-field microscopy examination of culture fluid for filamentous organisms. The causative organism is normally identified by growth inhibition tests and/or immunofluorescence test. Closely related Mycoplasma spp. may cause cross-reactions in these tests. Several new techniques that may overcome this problem are being developed and these include immunoblotting, immunoperoxidase and polymerase chain reaction (PCR) tests
Antigen detection
There are several antigen detection tests that may be useful in the confirmatory diagnosis, particularly in circumstances where good enough diagnostic samples cannot be collected for isolation of the organism. These include:
- Agar gel diffusion test - a practical and easy to perform test - may be used for the rapid detection of specific antigens in pleural fluid or ground lung tissues. A variation of this is the interfacial precipitation test.
- Indirect fluorescent antibody test, which can be applied on smears of pathological material using hyperimmune cattle serum against MmmSC and labelled anti-bovine IgG. The test is best used for smears of pleural fluid, although lung impression smears may also be used. The specificity of the method can be improved by counterstaining smears with Eriochrome black.
- Immunohistochemistry. MmmSC immunoreactive sites can be detected in the small bronchioles and alveoli and within the interlobular septa of lung lesions using the peroxidase-antiperoxidase (PAP) method on sections of paraffin embedded blocks. This is labour-intensive, but very useful, particularly on animals that die suddenly of an acute infection.
- PCR is currently more of a research tool than a diagnostic test that can be routinely applied.
Antibody detection
At present, complement fixation (microtitre method) (CFT) is the preferred serological test for CBPP. The specificity of this test can be as high as 99.5% in acutely infected cattle, but the frequency of false-positive reactions may temporarily be higher in certain herds. The sensitivity of the test is limited, and it may fail to identify four classes of animals:
- animals in the very early stages of the disease;
- animals in the very late stages of the disease (CFT fails to detect 30% of animals with chronic lesions);
- animals with massive lesions, where the antibodies produced are overwhelmed by the antigen; and
- animals that have been treated with antibiotics in the early stages of the disease, which may fail to develop a detectable serological response.
The CFT reaction after vaccination is inconstant and short-lived (generally less than 3 months). The CFT is generally used as a herd test.
The competitive enzyme linked immunosorbent assay (c-ELISA) has been evaluated under field conditions in several African countries, with the assistance of the International Atomic Energy Agency (IAEA). It is at least as sensitive as the CFT, but as with other ELISA systems, increased sensitivity can only be achieved at the expense of specificity, and vice versa. It is a useful tool to measure the antibody levels on a herd basis.
The passive haemagglutination test, while not used routinely, may have a place in serological diagnosis. It is more sensitive than the CFT in early and late stages of disease, but the specificity is lower. It has a potential role as a screening test.
The slide agglutination test is simple to perform and could be used as a pen-side test. It is more sensitive in the early stages of the disease, but it lacks specificity.
![]()
![]()
![]()
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}