![]()
![]()
![]()
Participation communautaire à un programme nutritionnel dans une région aride du Kenya
Participación comunitaria para mejorar la nutrición en zonas de sequía de Kenya
N.O. Bwibo, R. Biteyi and S. Kilobia
N.O. Bwibo, a former professor of paediatrics, is the Deputy Director General (Technical) of the African Medical and Research Foundation (AMREF). Robina Biteyi, a public health nurse, is Project Leader for AMREF's Kibwezi Rural Health Scheme. Susan Kilobia, an agricultural extension officer, is the coordinator of the Applied Nutrition Programme in Kibwezi.
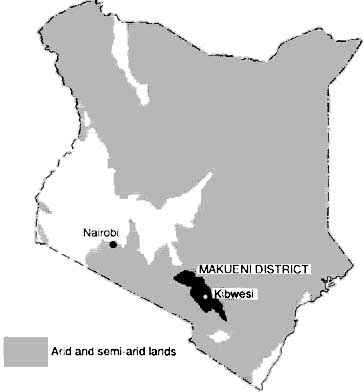
In Kenya, some of the poorest families reside in areas where the rainfall is low and unreliable, Kibwezi, a division of Makueni District of Kenya (see map), is located within the region known as the Arid and Semi-Arid Lands (ASALs). Approximately 200 km from Nairobi, Kibwezi is about 3 400 km2 in size with an estimated population of 170000. The main crops are maize, beans, cowpeas and pigeon peas, Millet, sorghum, cassava and sweet potatoes are grown by a few households. In spite of the area's rich, dark volcanic soils, low rainfall affects the agricultural output and there are frequent crop failures.
Makueni District, Kenya - District de Makueni (Kenya) - Distrito Makueni, Kenya
In 1984, Kibwezi faced one of the worst droughts and famines in its history. At the time, the African Medical and Research Foundation (AMREF) was operating an integrated primary health care (PHC) programme in the area, and nutrition was a critical element in the programme, AMREF is a developmental non-governmental organization (NGO) in East Africa serving the health heeds of communities, particularly those in remote, difficult-to-reach areas such as Kibwezi. While AMREF focuses on reaching people directly, it also works in close partnership with ministries of health, AMREF's work in Kibwezi illustrates a multisectoral approach to improving nutrition and the endeavours of an NGO to empower and support communities to develop the capacity to look after their health.
APPLIED NUTRITION PROGRAMME
When the famine occurred, an emergency feeding programme was carried out to stop further deterioration in the nutritional status of young children. The supplementary feeding programme lowered the rate of malnutrition among children under five years of age from 40 percent in October 1984 to 20 percent in June 1985. Yet there was an urgent need to find more appropriate ways of addressing the basic causes of malnutrition in Kibwezi. Recognition of this heed led to the initiation and implementation of the Applied Nutrition Programme (ANP) in 1986.
The ANP aimed to improve the nutritional status of young children, especially to reduce severe and moderate malnutrition from 29 to 14 percent. Other objectives were to raise production of drought-resistant crops from 37 to 57 percent; to increase production of rabbits from 7.4 to 10 percent; and to increase the number of birds per family from 13 to 20. In addition, 14 tree nurseries were to be established among 14 schools in Mtito Andei and Makindu. Support was given for the construction of energy-saving stoves and for two production units among 20 women's groups. Through participatory efforts, 100 water tanks were to be constructed in Mtito Andei and Makindu. Finally, six women's groups were to be assisted in initiating and managing income-generating activities.
An integrated approach was taken to address health, nutrition, household food security and income-generation objectives, using the following strategies: intersectoral collaboration; information, education and communication (IEC); capacity building of the community's own resource people (CORPs); and a revolving loan fund.
COMMUNITY PARTICIPATION
Community involvement was a guiding principle in implementing activities to reduce malnutrition. Through participation, people develop their capabilities and feel more self-reliant; thus activities can be sustained over time. One common definition (Rifkin, Muller and Bichman, 1988) states: "Community participation is a social process whereby specific groups with shared needs living In a defined geographic area actively pursue identification of their needs, take decisions and establish mechanisms to meet these needs. In the context of PHC this process is one which focuses on ability of these groups to improve their health care and by exercising effective decisions to force the shift in resources with a view to achieving equity". The 1986 National guidelines for primary health care in Kenya (Bennet and Maneno, 1986) define community participation as a "process by which a community mobilizes its resources, initiating and taking responsibility for its own development activities and sharing in decision making for and implementation of all other development programmes for overall improvement of its health status". In tackling Kibwezi's nutrition problems, the communities participated in all stages of programme development and implementation, as described below.
PROBLEM IDENTIFICATION
Through community meetings, people were mobilized to identify problems related to poor nutrition and to determine the magnitude of malnutrition in Kibwezi. Through women active in the community, self-help groups and religious and village leaders, AMREF staff were introduced to the local men and women. The leaders held several meetings and eventually identified four major problems: poor food security at household level, lack of income-generating activities, inadequate safe water and malnutrition among the young children.
When the leaders were asked to identify the causes of malnutrition among the young children, they first called attention to inadequate knowledge of good feeding practices. Second, they noted that women's heavy work load left them little time for child-rearing, nutrition and other activities. One village elder said. "Our women are extremely busy during planting season; as a result children are not fed as often as they should be". The third factor contributing to malnutrition was the high incidence of childhood illnesses (i.e. diarrhoeal diseases, measles and respiratory infections), which affected food intake. Finally, food insecurity at the household level led to poor nutritional status among children.
Late weaning, nutritionally inadequate feeding and withholding of food from children with measles or diarrhoea were inappropriate practices noted by the community. This information was very valuable for planning community health education sessions and for training community health workers (CHWs) and traditional birth attendants (TBAs).
It was interesting and rewarding to note that there were no misconceptions as to the causes of malnutrition, so the basis for health education was good. Furthermore, the community's views of the causes of malnutrition were very similar to those identified by the project staff (see figure).
PROBLEM ASSESSMENT AND RESOURCE MOBILIZATION
The next stage was to involve the community in assessing the scope or magnitude of malnutrition, CHWs were briefly trained in the use of a Shakir strip, a simple technology to measure mid-upper-arm circumference. With initial supervision, they measured mid-upper-arm circumferences of all children under five years of age, and 30 percent were found to be mildly or severely wasted. This information was shared with the communities, and the leaders agreed that malnutrition was becoming a serious problem for the communities and their children and that something had to be done about it.
Meetings were organized to plan how best to approach the problem. Community leaders, women's groups, CHWs, TBAs, schoolteachers and children were selected as the most appropriate people to obtain the skills needed to carry out community activities. The communities assembled resources for meetings, materials and nutrition activities. Schools as well as individual households provided land for agricultural activities.
PLANNING AND IMPLEMENTATION
Awareness-raising activities and discussions were held about the roles of the community groups and the implementation and sustainability of the activities. The community's identification of problems as well as other social and cultural factors, for example eating habits and beliefs, were the basis for the interventions.
Community mobilization and nutrition education were planned to instil good nutrition practices. Actions were initiated to assess, monitor and survey the nutrition situation, and malnourished children were rehabilitated. To improve household food security, community members were educated about food production, and income-generating activities were promoted, particularly those that could reduce women's workload.
Nutrition education
A learner-centred, problem-posing, self-discovery, action-oriented (LePSA) methodology of adult teaching (Freire, 1973) was used to approach nutritional problems (such as late weaning, infrequent feedings of foods low in nutrients, and withdrawal of foods, especially those high in protein, during measles or diarrhoeal episodes) identified during the initial dialogue between AMREF staff and the communities and through studies carried out in Kibwezi. Emphasis was put on the need for frequent feeding and preparation of nutritionally balanced feeds. Undesirable practices, especially withdrawal of certain foods during illness, were discouraged.
Nutrition assessment, monitoring and surveillance
Discussions of nutrition assessment, monitoring and surveillance of young children addressed some of the methods communities use to determine how well children are growing. For example, a child might be lifted to determine whether he or she is gaining or losing weight. A band worn by the child around the arm or hips indicates growth as well; if the band becomes tight, the child is gaining weight. After finding a parallel between their own traditional concepts of child growth monitoring and the modern concepts of weighing children and measuring mid-upper-arm circumference, the communities became interested in initiating their own child growth monitoring centres.
Two parameters, weight for age and mid-upper-arm circumference, were used by CHWs in assessing nutritional status and monitoring malnourished children. The project provided Salter scales and trained the CHWs in weighing children, plotting their weight on a health card and interpreting the weight as well as in taking upper-arm circumference measurements. They were also trained in counselling individual families. Community leaders and CHWs mobilized their communities in identifying venues for assessment and in acquiring stationery.
Rehabilitation of malnourished children
To rehabilitate malnourished children in the community, parents were encouraged to participate in the weekly monitoring of their children's weight gain and were shown ways to prepare high-energy, high-protein feeds; children were screened and referred for immunizations; and breast-feeding was promoted. Families with children who did not gain weight within three months were considered to be at high risk, and these children were followed more closely by CHWs and TBAs. Children who failed to gain weight were referred to a health facility or an outreach clinic for the opinion and management of a professional health worker.
Improvement of household food security
Skills training is provided to all the leaders, CHWs, TBAs, women's groups, teachers and pupils using the LePSA methodology noted above. Training covers promotion of drought-resistant crops, provision of seed loans, appropriate grain storage and preservation techniques and production of cheap animal protein, e.g. rabbits and poultry.
Since Kibwezi is prone to frequent famine and drought, an early warning system for detection of such problems has been developed to make possible timely and appropriate action to minimize their effects (see box). This system is a result of joint efforts between communities and intersectoral extension workers. It is based on traditional community experiences and proven scientific factors.
|
DROUGHT EARLY WARNING SYSTEM INDICATORS USED IN KIBWEZI · Abundant fruits on baobab, acacia and mango trees · A few flowers on the baobab · Prolonged rains in the coastal region · Patchy clouds accompanied by thunder and lightning prior to onset of rainfall · Ten-year cycle · Grouping of stars before the rains, with more stars in the group on the sunset side than in the group on the sunrise side · Windy and cold September (prior to the rainfall month) · Two consecutive good harvests in the long season |
Income-generation activities
Income-generation activities, particularly activities that would reduce women's workload, were promoted among women's groups. The women use newly acquired skills doing simple feasibility studies, simple bookkeeping and leadership and group management. For instance, two groups of women were trained in small business management. Through a loan repayment scheme, both groups were able to borrow money to purchase maize milling machines. The first group borrowed KSh 48000 (US$ 1920); it has repaid the loan and the business is now self-sustaining.
MONITORING AND EVALUATION
The CHWs collect baseline information on all the children under five years old in their area. They identify all homes with children in this age group, count the total number of children and note their ages and their immunization status.
CHWs in each growth-monitoring centre keep the following information on a monthly basis: the number of children who attend growth-monitoring sessions; the age, sex and village of the children; their weight and arm circumference; and the action taken. The CHWs use this information to determine whether they are reaching their target and to identify high-risk children for closer follow-up or referral. The CHWs analyse the data and inform the community through meetings. Simple quantitative methods are used in presenting results; for example, orange sections are used to explain the proportion of malnourished children.
Because of the slowness of changes in food traditions, habits and customs, any meaningful evaluation of the programme should be conducted after at least five years. Evaluation will be done using participatory methodology and focus-group discussions. The communities will be involved in planning and carrying out the evaluation activities to determine whether the objectives have been achieved.
CONSTRAINTS AND PROBLEMS
In spite of Kenya's long-standing self-help movement, some people continue to expect hand-outs, having become used to them in other projects. The first step in motivating people to participate is defining the concepts of dependency and sustainability, looking at the community's strengths and capabilities and seeing what people can do for themselves. With the community, AMREF identifies those areas where people think they heed help. Finally, it is necessary to look at causes of dependency and its effects.
Collection and analysis of information is time consuming, and finding time is a sacrifice for the CHWs, who are volunteers. It is difficult to calculate the amount of time spent on information collection because CHWs have different numbers of households under their care and the distance between households varies. However, experience shows that most CHWs spend at least a full day visiting their communities, and when they have to collect complete information they need another day and a half. Therefore, designing and implementing an adequate but simple monitoring system is still a very big challenge.
Community participation is community empowerment. Sometimes the recognition that is being accorded to communities and their ability to manage activities has been resented by professionals who considered these matters to be their domain. However, there has been considerable change in this attitude among professionals.
ACCOMPLISHMENTS
The implementation of ANP activities in Kibwezi has already produced tangible results, which are recognizable in the areas of growth monitoring, community empowerment and changes in infant feeding and food production practices. At the beginning of the project, prior to mobilization of the community, 483 children aged 36 to 59 months were measured and monitored by stationary and mobile clinics. As a result of community participation, 667 children in the same age group have been monitored in their own community by their own community members. In 1993 the number is on the rise. Until now, these vulnerable children have been difficult to reach because after completing the immunization schedule they attended the clinic less regularly or stopped attending completely.
Community participation in nutrition activities has given people confidence and empowered them to venture into other activities. For example, one community has initiated a community resource centre which keeps and lends reading materials on nutrition, food production and health.
Weaning diets developed with the people's participation are increasingly being utilized in the community. Previously introduced weaning diets, e.g. soybean mixtures, were not adopted because they did not use foods that were commonly grown and available in Kibwezi households.
Progress has been made in food production. Communities have established multiplication centres for cassava. Clean planting materials are now obtainable within the community. The proportion of farmers growing drought-resistant crops such as millet, sorghum, cassava and green gram is higher because of revolving seed loans, initiated and managed by the community.
Schools have initiated activities such as gardening and rearing of rabbits. Through the pupils, these activities have now filtered into the community. The communities at large are learning from their own children.
LESSONS LEARNED AND CONCLUSION
Community participation should be promoted right from the initiation of a nutrition programme. If promoted later, it meets with resistance and an already-established culture of dependence which is difficult to break. Considerable effort is required to build the capacity to make community participation in nutrition truly effective and sustainable.
In promoting community participation, both the real and felt needs of the community need to be addressed. An entry point or need that is meaningful to the community must be identified and used. Nutrition may not be a good entry point in certain communities; food production or activities to generate women's income may be better entry points, and their relationship with nutrition can then be emphasized. Food production should be given a priority in the quest for improvement of the nutritional status of the communities.
Nutrition problems are deeply ingrained in people's way of life, and fundamental changes need to take place before any lasting impact can be seen. Therefore, the priority of any nutrition project should be to develop the community's own resource persons, people with skills and expertise who can assist other community members in support of good nutrition.
Use of the at-risk approach, in which risk variables are defined and used to identify high-risk individuals and groups who require special attention, is important for targeting the most vulnerable families and making the best use of limited resources. In ANP the risk variables included single parenthood, family size, birth intervals, immunization status and landownership. Targeting high-risk families is one way of promoting their participation.
Several sectors are involved in nutrition, and collaboration among them is very important. Collaboration will minimize replication and mobilize resources for a concerted effort. In Kenya, the sectors include agriculture, livestock, water, social services and health. In these areas AMREF has been a facilitator rather than an implementing agency, focusing on building the capabilities of the community and supporting development of extension personnel.
REFERENCES
Bennet, F.J. & Maneno, J., eds. 1986, National guidelines for implementation of primary health care in Kenya. Nairobi, Ministry of Health, Government of Kenya.
Freire, P. 1973. Education for critical consciousness. New York, Seabury Press.
Rifkin, S.B., Muller, F. & Bichman, W. 1988, Primary health care: on measuring participation. Soc. Sci. Med., 26(9): 931-940.
La région de Kibwezi fait partie des terres arides et semi-arides du Kenya. Le manque de pluie est fréquemment à l'origine de mauvaises récoltes et les cycles de famine et de sécheresse reviennent tous les sept ou huit ans.
L'AMREF (African Medical and Research Foundation), organisation internationale indépendante, a but non lucratif, s'efforce d'améliorer l'état de santé de la population de Kibwezi depuis 1979. Elle a entrepris un projet de nutrition appliquée en 1986, pour aborder le problème de la malnutrition par une approche intégrée englobant la santé, la production alimentaire, la nutrition et la création de revenus. Le principe de base de ses activités est la participation communautaire. L'AMREF a assuré la participation des collectivités à l'identification des problèmes, à leur évaluation, à la planification, à la mobilisation des ressources, à l'exécution, la surveillance et l'évaluation des activités.
La participation communautaire est déterminante pour la mise en valeur des capacités locales et la poursuite des activités au-delà de la phase de financement. Elle est encouragée par la mobilisation collective, la sensibilisation du public et le renforcement des capacités des collectivités. Il y a eu quelques résultats: l'amélioration de la surveillance de la croissance des jeunes enfants dans les collectivités. Ce groupe d'âge reste hors d'atteinte pour les centres de soins maternels et infantiles traditionnels. Des aliments de sevrage appropriés ont été mis au point avec les collectivités à partir de produits locaux. Ils sont de plus en plus souvent utilisés. On a augmenté la production de cultures résistant à la sécheresse telles que manioc, mil, sorgho et céréales vertes. Les écoles se sont lancées dans la promotion de la production alimentaire.
En conclusion, on peut dire que la participation communautaire profite autant aux collectivités qu'à l'AMREF. Les enseignements tirés de ce projet aideront l'AMREF et les collectivités à planifier leurs stratégies futures.
La Región de Kibwezi forma parte de las tierras áridas y semiáridas de Kenya. La escasez de lluvias provoca a menudo cosechas deficientes, por lo que se han producido períodos de carestía y sequía aproximadamente cada siete u ocho años.
La Fundación Africana para la Medicina y la Investigación (AMREF), organización internacional independiente y sin fines de lucro, trabaja desde 1979 para mejorar el estado de salud de la población de Kibwezi. En 1986 puso en marcha un proyecto de nutrición aplicada para tratar de solucionar el problema de la malnutrición con un planteamiento integrado que aborda las cuestiones de la salud, la producción de alimentos, la nutrición y la generación de ingresos. El principio en que se basan sus actividades es el de la participación comunitaria con el fin de garantizar la participación de las comunidades en la determinación de los problemas, su evaluación, la planificación, la movilización de recursos y la ejecución, la vigilancia y la evaluación de las actividades.
La participación de la comunidad se considera fundamental para fomentar la capacidad local y mantener las actividades después del período de financiación, y esta enormemente apoyada por la movilización comunitaria, el fomento de la toma de conciencia y la creación de capacidad. Se han alcanzado algunos logros, entre los que cabe destacar; el aumento de la vigilancia del crecimiento de los niños pequeños, que era difícil de atender a través de los centros de salud maternoinfantil; la preparación y creciente utilización de dietas de destete adecuadas utilizando alimentos locales, en la que han colaborado las comunidades; el aumento de la producción de cultivos resistentes a la sequía, como por ejemplo, la yuca, el mijo, el sorgo y los cereales verdes; y, en las escuelas, la puesta en marcha de actividades que fomentan la producción de alimentos.
La participación comunitaria beneficia tanto a la comunidad como a la AMREF y los conocimientos adquiridos gracias a este proyecto serán de ayuda a ambos para planificar su estrategias para el futuro.
![]()
![]()
![]()
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}